Need of Calcium and Vitamin D in Patients after a Recent Fracture ()
1. Introduction
Patients older than 50 years presenting with a fracture have an increased risk for subsequent fracture, which is highest during the first years after a fracture [1-8]. Therefore, medical therapy is advocated in fracture patients at high risk of subsequent fractures, including drug therapy and adequate intake of calcium and vitamin D [9-13]. Regardless of fracture history, calcium intake is low in subjects older than 50 years, in the elderly and in patients with osteoporosis [14-16]. Vitamin D insufficiency (serum 25(OH)D concentration <50 nmol/l) is endemic worldwide [17] and is frequently present in patients with osteoporosis, with or without a fracture [18-31]. There is large heterogeneity in the medical literature about the clinical approach to determine the need and amount of calcium and vitamin D supplements [9-34]. Clinical trials with fracture prevention as endpoint used variable doses of calcium (0 - 1500 mg/d) and vitamin D supplements (250 - 1200 IU/d), in some studies at fixed doses and in other studies according to baseline levels [35-37]. In guidelines on osteoporosis, the clinical standard for measuring the need of calcium is to evaluate calcium intake (such as by interview or standard questionnaires) [9-13,35-37]. A total calcium intake of at least 900 - 1500 mg/d is advocated to be achieved by diet or by calcium supplementation when necessary [9-13,20-22, 27-31]. In these guidelines, the upper limit of advised calcium intake varies, as far as mentioned, between 1200 and 2500 mg/d [12,22,27]. All osteoporosis guidelines advocate fixed supplements between 400 and 1200 IU D3/d [9-13]. In addition, one guideline advocates measurement of serum levels of 25-hydroxyvitamin D (25 (OH)D) in elderly when osteomalacia or when vitamin D deficiency is suspected [12]. Desirable serum levels of 25(OH)D is not mentioned in one guidelines[11], or specified in others as 50, 75 or 80 nmol/l [9-13]. In the context of fall prevention and prevention of non-vertebral fractures, even serum levels of 100 nmol/l are considered as desirable levels [32-34,38]. There appears to be no evidence that it would be beneficial to increase serum 25(OH)D levels above 150 nmol/l [30]. In terms of safety, a vitamin D intake of 2000 IU/d [22,32-34,38], and even up to 10.000 IU/d is considered as safe [38,39]. In terms of serum concentrations of 25(OH)D, the upper limit of safety is 220 nmol/l [33,38] or even 374 nmol/l [40]. It takes approximately two to three months to achieve desired serum levels, [40] but the exact relation between specific dosing regimens of vitamin D supplements and the timing needed to achieve desired levels is unclear [30,38]. We evaluated the calcium intake and serum 25(OH)D levels in patients at the time they presented with a fracture and calculated the supplements needed to achieve desirable levels, taking into account upper safety levels.
2. Methods
Of the 902 consecutive patients, who were enrolled in a study to evaluate the prevalence of contributors to secondary osteoporosis, 502 were available for prospectively planned evaluation (Figure 1).
Patients known to have an active malignancy or recent chemotherapy, end-stage renal disease, high-impact trauma, need for critical care services, a history of gastrictomy, small bowel resection and eating disorders (n = 10) were excluded. Other reasons for non-participation were not being able to show up at the measurements or no interest in fracture risk evaluation (n = 237), no results of serum calcium (n = 20) or 25(OH)D (n = 2), primary (n = 17) or idiopathic hyperparathyroidism (n = 8) (serum PTH was measured in all), hypercalciuria (n = 4) (calciuria was measured on indication in 16 patients) and non-response to calcium questionnaire (n = 102). Dietary calcium intake was ascertained from a food frequency

Figure 1. Flow chart of included patients presenting with a fracture.
questionnaire completed by the subjects and then reviewed by the physician during the office visit. Total calcium intake was calculated as average daily dietary calcium intake from this questionnaire plus 250 mg/d as standard intake from background diet [12]. Serum 25(OH)D concentration was measured immunochemically using the LIASON® assay (DiaSorin, Saluggia, Italy). Bone mineral density (BMD) in the left or right hip and the lumbar spine was determined using dual Xray absorptiometry (DXA) with the Hologic QDR 4500 (Hologic Discovery Corp, Waltham, MA, US). Diagnosis of osteoporosis was based on the criteria of the World Health Organization (WHO) for BMD [41] as provided by the manufacturer for women and men [41].
Fractures were grouped in hip, major (clinical vertebra, pelvis, distal femur, proximal tibia, multiple rib, and proximal humerus), minor (all remaining fractures, excluding fingers and toes) and fingers and toes [1].
We analyzed the effects of several doses of calcium supplementation (500 and 1000 mg/d) and of vitamin D supplementation (400, 800, 1200, 1600, 2000 and 2400 IU D3/d), as currently available in the Netherlands for daily practice.
Based on the baseline calcium intake, we calculated the percentage of patients who needed individualized doses of 500 mg/d or 1000 mg/d of calcium to achieve a total calcium intake of 1000 or 1200 mg/d. Based on baseline serum levels of 25(OH)D, we calculated the percentage of patients who needed 800 IU/d or more of vitamin D supplements to achieve serum levels of 25(OH)D of 50 or 75 nmol/l, taking into account that serum levels would raise by 1.2 nmol/l per 40 IU/d if baseline 25(OH)D levels are <50 nmol/l [38]. We furthermore analyzed the effects of systematic supplementation of several fixed doses of calcium and vitamin D supplements to all patients. We calculated the percentage of patients who would surpass the upper limit of safety when using individualized and systematic fixed doses (defined as a calcium intake > 1500 mg/d [12] and serum concentrations of 25(OH)D >220 nmol/l). Multivariable analysis was performed to investigate whether age, sex, BMD and fracture location at baseline were related to baseline calcium intake or baseline serum levels of 25 (OH)D. ANOVA was used for analysis of seasonal variations in term levels of serum 25(OH)D concentrations.
3. Results
Baseline characteristics of fracture patients are shown in Table 1.
Mean calcium intake was 839 mg/d (range 250 - 2050 mg/d) and mean serum 25(OH)D concentration was 43 nmol/l (range < 10 to 130 nmol/l). The combination of a calcium intake of ≥1000 mg/d and a serum 25(OH)D concentration of ≥50 nmol/l was present in 11% of the patients. The combination of a calcium intake of <1000 mg/d and a serum 25(OH)D of <50 nmol/l was present in 43% of the patients (Figure 2). None of the patients had a calcium intake of ≥1200 mg/d together with serum 25(OH)D levels of ≥75 nmol/l. We checked the representativity of the participating population. Patients in the non-participating group were significantly older (74 years versus 70 years, p < 0.001) and had more major (35% versus 30%, p < 0.001) and hip fractures (18% versus 8%, p < 0.001) compared to the patients that were eligible for this study.
3.1. Calcium Intake
The individualized doses of calcium supplementation

Table 1. Patient characteristics (n = 502).

Figure 2. Baseline daily calcium intake and serum 25-hydroxyvitamin D levels in 502 patients older than 50 years at the time they present with a fracture. Number and % of patients are given for the four quadrants. Only 55 (11%) patients achieved a daily calcium intake ≥ 1000 mg/day and a 25(OH)D level ≥ 50 nmol/l (green quadrant).
needed to achieve several desirable levels of total daily calcium intake based on baseline calcium intake are shown in Figure 3 (panels (a) and (b)).
In order to achieve an individualized total daily calcium intake of ≥1000 mg/d, 31% needed no calcium supplements, 57% needed supplementation of 500 mg/d and 12% needed 1000 mg/d. In order to achieve an individualized daily calcium intake of ≥1200 mg/d, 9% needed no supplements, 59% needed 500 mg/d and 32% needed 1000 mg/d. To achieve an individualized intake of 1500 mg/d, 31% needed 500 mg/d, 57% needed 1000 mg/d and 12% needed 1500 mg/d of calcium supple-
 (a)
(a)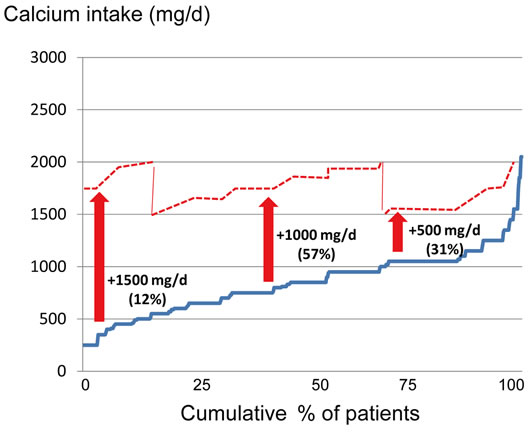 (b)
(b)
Figure 3. Effect of applying an individualized calcium dose supplementation strategy in order to achieve a total daily calcium intake of ≥1000 mg/d (panel (a)) and of ≥1500 mg/d (panel (b)) in patients older than 50 years with a fracture. Blue line: % of patients (X-axis) with the total amount of daily calcium intake (mg/day) at baseline (Y-axis). Blue dotted line: total daily calcium intake when using an individualized calcium dose supplementation strategy in order to achieve a total daily calcium intake of ≥1000 mg/d in all patients. Red dotted line: total daily calcium intake when using an individualized calcium dose supplementation strategy in order to achieve a total daily calcium intake of ≥1500 mg/d in all patients.
mentation.
When applying an individualized calcium dose supplementation strategy in order to achieve a total daily calcium intake of ≥1000 mg/d in all patients, only 1% of the patients would surpass a total daily intake ≥ 1500 mg/d. These patients already had an intake ≥ 1500 mg/d at baseline. When aiming at an individualized total daily calcium intake ≥ 1200 mg/d, half of the patients who needed 1000 mg/d calcium supplementation to achieve this goal would surpass 1500 mg/d. In the patients that needed 500 mg/d calcium supplementation in order to achieve a total daily calcium intake ≥ 1200 mg/d, 37% would also surpass 1500 mg/d.
If patients systematically would be supplemented with a fixed calcium dose of 500 mg/d, 85% would achieve a total daily calcium intake of 1000 mg/d, 67% of the patients would achieve an intake of ≥1200 mg/d and 31% of the patients would surpass a total daily calcium intake of 1500 mg/d. If patients systematically would be supplemented with a fixed calcium dose of 1000 mg/d, all would achieve an intake of 1000 mg/d and 1200 mg/d, and 88% of the patients would achieve a total calcium intake above 1500 mg/d (Figure 4).
Only sex was a risk factor for low calcium intake at baseline: mean calcium intake was lower in men than in women (B: −116, 95% confidence interval (CI): −179, −53). Calcium intake did not differ according to age (B: −0.4, CI: −3.0, −2.2), total hip BMD (B: −6.7, CI −20.4, 33.9) or fracture locations (overall p = 0.348), i.e. low calcium intake was as frequent in younger as in older patients, at all levels of BMD and at all fracture locations.
3.2. Serum 25(OH)D
In order to achieve an individualized serum 25(OH)D
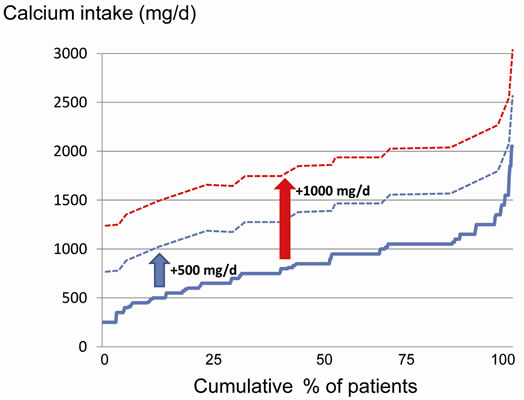
Figure 4. Achieved total amount of daily calcium intake when using a systematic fixed supplementation of 500 mg (blue dotted line) and 1000 mg (red dotted line) calcium per day in patients older than 50 years with a fracture. Blue line: cumulative % of patients (X-axis) with the total amount of daily calcium intake (mg/day) at baseline (Y-axis).
level of 50 nmol/l, 34% of the patients did not need vitamin D supplementation, 41% of patients needed 400 - 800 IU/d vitamin D3, 17% needed 1200 IU D3/d and 9% needed 1600 IU D3/d (Figure 5 panels (a)-(c)). To achieve an individualized calculated serum level of 75 nmol/l, 10% did not need D3 supplements, 22% needed 800 IU D3/d, 19% needed 1200 IU/d, 20% needed 1600 or 2000 IU/d and 9% needed 2400 IU/d. To achieve an individualized calculated serum level of 100 nmol/l, 5% needed 800 IU/d, 11% needed 1200 IU/d, 16% needed 1600 IU/d, 19% needed 2000 IU/d, 20% needed 2400 IU/d and 28% needed higher doses than 2400 IU/d.
If all patients systematically were prescribed supplements of 800 IU D3/d, 75% of the patients would achieve a level ≥50 nmol/l, 33% a level ≥75 nmol/l and 9% a level ≥100 nmol/l (Figure 6). If all patients systematiccally were prescibed supplements of 2000 IU D3/d, all patients would achieve levels ≥50 nmol/l, 90% a level ≥75 nmol/l and 50% a level ≥100 nmol/l. None of the calculated individualized or systematic vitamin D supplements would bring serum 25(OH)D above the toxic level of 220 nmol/l.
Risk factors for low serum 25(OH)D were being female (B: 5.6, CI 0.8, 10.5), increasing age (B −0.5, CI: −0.3, −0.7) and low BMD (B: −2.9, CI: −0.7, −4.9). Mean serum 25(OH)D was similar between major, minor or finger and toe fractures (overall p = 0.575).
Mean serum levels of 25(OH)D significantly varied during the year, being lowest in January (28 nmol/l, range: 0 - 66 nmol/l) and highest in August (55 nmol/l, range: 16 - 95 nmol/l) (p < 0.0001 by ANOVA).
4. Discussion
The baseline levels of calcium intake and serum 25 (OH)D varied widely between fracture patients. Consequently, the need and amount of supplements varied between fracture patients.
A combination of adequate calcium intake and serum 25(OH)D was low, even if the most conservative levels were considered: only 11% of patients had a calcium intake of ³1000 mg/d and serum 25(OH)D of ³50 nmol/l, indicating that the large majority of patients needed calcium and/or vitamin D supplements according to currently available guidelines. These results confirm that vitamin D deficiency is endemic in the Netherlands (as elsewhere in most parts of the world), and that the combination of vitamin D deficiency with insufficient calcium intake is common in fracture patients, at least in the Netherlands. However, the doses of needed calcium and vitamin D supplements is not only guided by baseline levels, but also by desirable levels, upper safety levels and the decision of application of individually titrated or fixed supplements to all fracture patients. As a result,

Figure 5. Effect of applying an individualized supplemental D3 dose in order to achieve a desired serum 25(OH)D level: ≥50 nmol/l (green line) in panel (a), ≥75 nmol/l (orange line) in panel (b) and ≥100 nmol/l (red line) in panel (c). Blue line: baseline values of serum 25(OH)D levels (Y-axis, nmol/l) in cumulative % of patients (X-axis).
calculation of adequate supplement doses in daily practice, whether individualized or at the group level, was much more complex than originally expected.
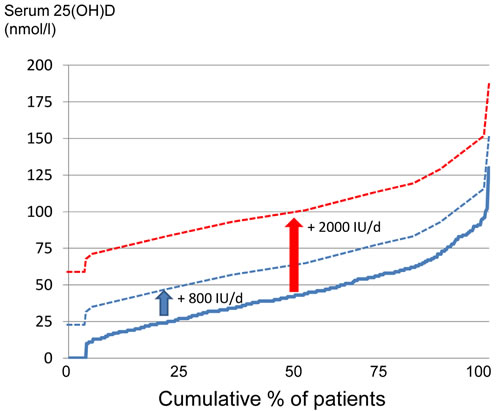
Figure 6. Achieved 25(OH) D levels when using a fixed supplemental D3 dose of 800 IU/d (blue dotted line) and 2000 IU/d (red dotted line). Blue line: baseline values of serum 25(OH)D levels (Y-axis, nmol/l) in cumulative % of patients (X-axis).
4.1. Calcium
The baseline calcium intake, and therefore also the need for calcium supplementation, was very heterogeneous in fracture patients. Mean calcium intake was lower in men than in women, but was not related to age, BMD, or baseline fracture location. This indicates that calcium intake should be checked in all fracture patients, and when necessary, the calcium intake should be increased by diet or supplements.
In order to achieve individualized total calcium intakes between 1000 and 1500 mg/d, 12% needed 1000 mg/d, 57% needed 500 mg/d and 31% needed no calcium supplements. In order to achieve calcium intake between 1500 and 2000 mg/d, 12% needed 1500 mg/d, 57% needed 1000 mg/d and 31% needed 500 mg/d of calcium supplements.
Prescribing a fixed supplement dose of 500 mg/d of calcium would be insufficient to achieve an intake of 1000 mg/d in 12% of the fracture patients, but it would raise the calcium intake to 1000 - 1500 mg/d in 57%, and to ≥1500 mg/d in 31% of fracture patients. In fracture patients, a fixed supplement dose of 1000 mg/d would raise the total calcium intake to 1000 - 1500 mg/d in 12%, to 1500 - 2000 mg/d in 57% and to ≥2000 mg/d in 31% of them.
The upper maximal limit for calcium intake is unclear and a matter of debate [42,43]. From a physiological point of view, an intake of more than 1200 mg/d, especially more than 1500 mg/d, does not further increase net calcium absorption in combination with adequate vitamin D supplementation, and therefore is considered unnecessary [44]. In terms of safety, the upper limit of intake is considered 1500 - 2500 mg/d [22,27,45]. However, an intake of more than 1200 mg/d is already considered as possibly unsafe in view of the possibility of increased risk of CV events [12]. The increased risk of CV events has been shown in healthy postmenopausal women and men with a mean baseline intake of 800 mg/d, who received calcium supplement of 1000 mg/d [46,47]. However, such side effects were not found in other studies and were not prospectively studied as primary or secondary endpoint [48], which still leaves open the question as to which is a safe upper level of calcium intake [42, 43].
In daily practice, taking into account the guidelines, calcium supplements should be titrated individually in order to achieve a total calcium intake between 1000 and 1500 mg/d in all patients. In our study this can be achieved easily with calcium supplements of 1000 mg/d in 12% of the patients with lowest baseline calcium intake and with 500 mg/d in 56% of the patients with moderate baseline calcium intake, while 31% did not need calcium supplementation. It is of interest that cross-sectional studies show that a neutral calcium balance is achieved at an intake of 741 mg/day of calcium [15]; and that, if vitamin D serum levels are adequate, the need of total calcium intake would be lower than 1000 mg/d [44]. However, such hypotheses still need to be tested prospectively.
4.2. Vitamin D
The baseline levels of 25(OH)D, and therefore, the need of vitamin D supplementation was also very heterogeneous in fracture patients. Lowest serum levels of 25(OH)D were found in elderly (>70 years) fracture patients with osteoporosis, in patients with a hip fracture, in 50 - 70 year old patients, during winter and summer time and in patients with other fractures than hip fractures, indicating the need for vitamin D supplements in all fracture patients.
In order to achieve serum levels of ≥50 nmol/l in all patients, more than half of the patients needed individually titrated doses between 400 en 1600 IU D3/d. In order to achieve serum levels of ≥75 nmol/l in all patients, 90% of the patients needed individually titrated doses between 800 en 2400 IU D3/d. In order to achieve serum levels of 100 nmol/l, all patients needed individually titrated doses between 800 en 3200 IU D3/d.
In fracture patients, a fixed daily vitamin D dose of 800 IU D3 would be sufficient to reach 50 nmol/l in 75%, to reach 75 nmol/l in 33% and to reach 100 nmol/l only in 9% of the patients, respectively. A fixed daily vitamin D dose of 2000 IU D3 would be sufficient to reach 50 nmol/l in all, but insufficient to reach 75 nmol/l in 10% and insufficient to reach 100 nmol/l in 50% of the patients.
None of the above mentioned individually titrated doses (400 to 3200 IU D3 daily) or fixed doses (800 to 2000 IU D3 daily) would raise serum levels of 25(OH)D above the toxic level of 220 nmol/l.
Therefore, based on the guidelines, the simplest clinically decision for most fracture patients would be to systematically prescribe 800 IU D3/d if the desirable level is 50 nmol/l and 2000 IU D3/d if the desirable level is 75 nmol/l, without needing measurements of baseline serum levels of 25(OH)D. However, the cost of this approach needs to be compared with the cost of measuring 25(OH)D and individualized use of appropriate calculated D3 doses.
Some experts argued that a fixed dose of vitamin D is sufficient [45], while others argued that the achieved serum level is crucial [38,44]. Another point of uncertainty is how long these doses of supplementation are needed. Presumably, it takes two to three months to achieve desirable serum levels [38,40,49]. However, it is unclear if at that time a follow-up measurement of serum 25(OH)D is indicated and how the dose can be adapted based on this follow-up measurement. Therefore, there is need of dose-effect studies focusing on vitamin D supplementation based on baseline values 25(OH)D levels, desirable serum levels and dose adaptation during follow up according to new measurements of serum 25(OH)D levels.
This study has several limitations. Firstly, the need of calcium and vitamin D supplements was calculated and not prospectively evaluated. Our analysis however tried to give considerations for current clinical practice based on current available guidelines, in attendance of prospective dose finding studies on this subject. Patients were treated with 800 IU D3/d without further measurement of serum 25(OH)D concentration, according to current guidelines in the Netherlands [50].
Secondly, the calculation of vitamin D supplements was based on the results of meta-analyses on dose-effect studies [38,44]. For calculating the effect of vitamin D3 supplementation on serum 25(OH)D concentration, a rise of the 25(OH)D level with 1.2 nmol/l for each 40 IU supplemental D3/d was taken into account, based on results found in patients with baseline values < 50 nmol/l [38,44]. In patients with baseline serum 25(OH)D > 50 nmol/l, the increase of 25(OH)D level would be 0.6 nmol/l per 40 IU supplemental D3/d, and therefore, these patients would have a more modest increase than patients with lower baseline intakes. However, there is a lack of studies with a randomized prospective design, specifically analyzing dose-effect of vitamin D3.
Thirdly, sun exposition and artificial UV exposition are other ways to provide supplements of vitamin D. These were not taken into account as the exact timing and dose of such ways of supplementation is unclear and difficult to evaluate in clinical practice [13].
Fourthly, only 58% of all fracture patients participated in the analysis. As in other studies, participation of fracture patients in follow up programs is low, which can be explained by early dead, dementia, co-morbidity, personal reasons, and decisions of family members, especially in the elderly [51]. There is need to improve this low response of fracture patients, as many patients with high fracture risk, such as after a hip fracture, are probably even more deficient in calcium and vitamin D intake [24].
Fifthly, the results of this study cannot be generalized to other countries, since the mean calcium intake and serum 25(OH)D concentrations are low in fracture patients in the Netherlands compared with other countries [5,19]. In the US, calcium intake is deficient [16], but intake of vitamin D3 supplements is higher than in Europe, because the allowed dosage of vitamin D3 in food is higher compared with European countries [12]. Therefore, the prescribed dosage of calcium and vitamin D3 supplements in fracture patients need to be adapted to regional baseline status of calcium intake and serum 25(OH)D. Furthermore, no calculations were made for vitamin D2 supplementation. This should also be calculated for countries were only vitamin D2 is available for supplementation.
In conclusion, the results of this study indicate that baseline values of calcium intake and baseline serum levels of 25(OH)D vary considerably in fracture patients. Taking into account desirable and safety amounts of calcium intake, desirable and safety serum levels of 25 (OH)D, the amounts of supplements to be given and the choice between individualized or systematic use of different doses, all these factors have to be carefully considered by the clinician who takes care of fracture patients. We propose that calcium and vitamin D supplements should be titrated on an individual basis according to the baseline values in combination with desirable need and safety levels. Supplementation of fixed dosages of D3 may result in suboptimal levels of vitamin D and fixed dosages of calcium may result in very high calcium intake, especially with a fixed dose of 1000 mg calcium. Further longitudinal studies are needed to answer questions regarding how to achieve and maintain optimal serum vitamin D levels and adequate calcium intake in fracture patients with either titrated or systematic fixed supplementation calcium and vitamin D dosages.