Adenoma of the Nipple, Mimicking Paget’s Disease of the Breast: Report of a Case ()
1. Introduction
Nipple adenoma is a rare benign neoplasm which originates from the nipple of the breast. In 1955 Jones described this first time as florid papillomatosis. Also this condition is known as erosive adenomatosis or superficial papillary adenomatosis. Although this is a benign tumor clinically it is very difficult to differentiate between malignant conditions like carcinoma and Paget’s disease of the breast [1] . Patient usually presents with subareolar nodule, pain, nipple discharge, erythema and ulceration Proper pre-operative diagnosis is essential because any misinterpretation of histopathological report can lead to undue mastectomy as reported by Carter et al. [2] .
2. Case Presentation
A 36-year-old woman presented with a history of a left sided bloody nipple discharge for one year duration. Subsequently she developed severe nipple ulceration. The patient was seen by a dermatologist and was given systemic antibiotics and local corticosteroids with no response. On physical examination, the left nipple was completely eroded with extensive skin ulceration. Otherwise, both breasts and axillae were clinically free with no palpable lymphadenopathy.
Clinical differential diagnoses included: Paget’s disease of the nipple and skin malignancy. However, nipple adenoma was not clinically suspected. Bilateral breast ultrasound and mammogram did not show any abnormality. Small incisional biopsy showed nipple adenoma. A complete excision of the eroded left nipple and part of the surrounded areola was achieved in addition to part of the retro-areolar breast tissue (Figure 1). Microscopically, the nipple showed lesion featuring complex ducts composed of bland oval cells with variable degree of hyperplasia which were focally continuous with squamous epithelium of the skin. The epithelial cells did not display any significant pleomorphism, mitotic activity or necrosis. Focal nipple ulceration is also noted (Figure 2 and Figure 3), without evidence of malignancy. The picture was consistent with nipple adenoma. Nipple reconstruction was planned at a later stage.

Figure 1. gross picture of the resected specimen including the eroded nipple, part of the areola and underlying breast tissue.

Figure 2. Complex ductal architecture underlying the surface epithelium with focal ulceration. (4× Low-power photomicrograph).
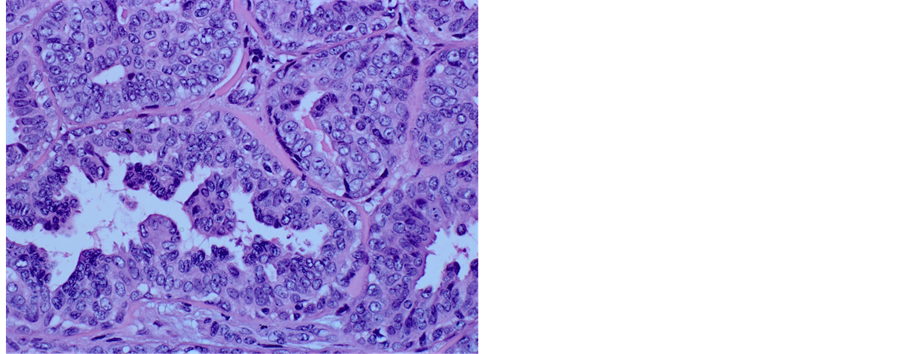
Figure 3. Ducts comprised of bland-looking epithelial cells with variable hyperplasia. (20× High-Power photomicrograph).
3. Discussion
Nipple adenoma, also known as florid papillomatosis, erosive adenomatosis or superficial papillary adenomatosis is a benign condition simulating malignancy such as breast carcinoma and/or Paget’s disease clinically [1]. Women in their 4th and 5th decades commonly affected and usually they presents with unilateral, serous or bloody nipple discharge in the presence of crusting. The main differential diagnosis is Paget’s disease of the nipple based on similar clinical features like soreness, ulceration and swelling of the nipple, sometimes with discharge [3] [4] . However, Paget’s disease is more common in older women and Paget’s cells can be detected by aspiration biopsy cytology. Whereas adenoma of the nipple tends to occur in premenopausal women.
The pathological characteristics of adenoma of the nipple are the maintenance of a double layer composed of epithelial and myoepithelial cells, no accompanying epithelial necrosis, and a definite direction of the duct cell arrangement in a pattern of pseudo invasion. It can be difficult to distinguish adenoma of the nipple from ductal carcinoma when the adenoma shows a marked proliferation of epithelial cells accompanied by pseudo invasion [5] . The coexistence of carcinoma and nipple adenoma has been noticed before by many investigators, and the reported incidence of this phenomenon varies in different studies. Fisher et al., found that, in a group of 967 patients with carcinoma, 1.2% had associated nipple adenoma [6] .
Nipple adenomas are papillary or solid adenomas developing within the nipple where proliferation of papillary epithelium is remarkable [2] [7] . The histological patterns of nipple adenoma are described by Rosen as adenosis, papillomatosis, mixed proliferative and sclerosing papillomatosis [8] .
There is no evidence of metastasis in this disease but local recurrences can occur when the neoplasm is incompletely excised. Hence, nipple reconstruction is usually planned after completeness of excision is confirmed histologically.
Bloody or serous nipple discharge is the most common presenting complaint in 65% - 70% of the patients, followed by enlargement and induration of the nipple associated with ulceration, which have been reported in medical literature [9] -[11] . However, histopathological evidence is medatory for the diagnosis of this rare condition. Afetab et al., described 19 cases of nipple adenoma over a period of 14 years; all patients were females with age ranging from 23 to 63 years. Most of the cases presented clinically with induration and ulceration. The diagnosis was clinically suspected in only 3 cases and the final diagnosis was confirmed by histology alone [12] .
Similarly, our patient presented with bloody nipple discharge associated with extensive erosion raising the clinical suspicion of Paget’s disease. Incisional biopsy was performed and histopathology report revealed a diagnosis, adenoma of nipple. Since complete excision is curative, local recurrence has been reported in 30% of incompletely excised lesions [13] , our patient underwent complete excision of the eroded nipple and part of the areola together with part of the retro-areolar breast tissue to achieve adequate excision and minimize local recurrence. The final histopathologic diagnosis showed adequately excised nipple adenoma.
In conclusion we report a rare case of nipple adenoma mimicking Paget’s disease of breast which is a diagnostic challenge. Nipple adenoma should be considered as a part of differential diagnosis when there is severe nipple erosion. Complete excision is the treatment of choice to avoid local reccurence.
Acknowledgments
We thank Dr. Abdul-Wahed Meshikhes, Consultant surgeon at Department of Surgery, King Fahad Specialist Hospital, Dammam 31444, Saudi Arabia, for revising the manuscript.
NOTES
*Corresponding author.