25 years’ experience in the management of pilonidal sinus disease ()
KEYWORDS
Pilonidal Sinus; Phenol Injection; Excision with Primary Closure; Excision with Packing
1. INTRODUCTION
In 1833, Herbert Mayo described a hair-containing sinus [1], but it was not until 1880 that Hodge [2] suggested the term “pilonidal” (Latin: pilus = hair and nidus = nest). By definition, a pilonidal sinus is a sinus that contains hairs, mainly in the sacrococcygeal area and is due to favoring conditions like: The existence of a deep natal cleft and the presence of hair within the cleft, sweating, maceration, bacterial contamination, and penetration of hairs [3]. In addition, certain effect exerted by the movement of the buttocks encourages loose dead hair to gain entry to the sinus [4]. This pilonidal sinus disease was also branded as “jeep disease” during the Second World War because of the high incidence among jeep drivers [5].
The origin of pilonidal disease is not fully understood. There are two theories associated with its pathogenesis: the acquired and the congenital theories. However, the majority of opinion favors the acquired theory, which postulates that the sacrococcygeal pilonidal infection originates in a natal cleft hair follicle that has become distended with keratin [6,7]. Even though the highest encounter of pilonidal sinus is in the postsacral region, other sites like the interdigital, axillary, umbilical, perianal, para-anal and intra-anal regions have been reported [8,9].
The onset of pilonidal sinus is rare before puberty and after the age of 40. Males are affected more frequently than females by a ratio of 3 to 1, probably due to their more hirsute nature [10]. Such condition is more common in Caucasians than Asians or Africans due to differing hair characteristics and growth patterns [11,12]. In the USA, the incidence of pilonidal sinus disease is 0.07% and is higher among men aged between 15 and 30 years [13,14]. In addition, data collected from the Office of Population Censuses and Surveys in England showed that on the average, about 7000 people were admitted to hospital every year for treatment of pilonidal sinus with a mean hospital stay of 4.3 days; one quarter of these were females [15,16].
Pilonidal disease is a common medical condition that accounts for almost 15% of anal suppurations and is responsible for much morbidity. Its treatment places a burden on hospital and community resources [17,18]. Many methods of treatment have been advocated to manage this disease, they include: phenol injection treatment, excision with primary closure and excision with packing (healing by secondary intention).
The excision of pilonidal sinus is facilitated, in general, by the injection of methylene blue dye via the primary or secondary orifices. The relative merits of these procedures, as used in 252 patients over a 25-year period, have been reviewed in this article.
2. MATERIALS AND METHODS
During the period between 1984 and 2009, two hundred and ninety-eight patients were treated for natal cleft pilonidal disease. Age, sex, presentation, number of sinus openings, treatment, complications, inpatient stay and outcome were recorded. Forty six patients (30 males and 16 females) presented as emergency with pilonidal abscess and two hundred and fifty two patients (168 males and 84 females) were referred with a chronic pilonidal sinus. Mean age at presentation was 25.5 years (range 17 - 69). Twenty-five patients had no follow up, disappeared and were excluded from this study resulting in 273 patients seen for pilonidal sinus. Twenty one patients were relieved with antibiotics, shaving the area and scrubbing it with tough loafe, while 88 patients of the remaining 252 were treated by excision and packing, 100 patients treated with excision and primary closure, and 64 patients received pure phenol injections (Table 1).
All patients treated with excision underwent general anesthesia and were positioned in a prone position with buttocks separated and held apart with adhesive tape. Elliptical incision was performed till we reached the presacral fascia.
On the other hand, the technique of phenol injection was performed according to Lord Millar technique under local anesthesia. It consisted of enlarging the fistula opening with forceps, scrapping out the debris and brushing the cavity to remove its contents [19]. Pure phenol was injected in the sinus, left for one to three minutes and then curetted; this was repeated 3 times. Patients treated by phenol injection were kept in hospital overnight and discharged home the following day with instructions to do sitz-bath daily and to keep the area shaved. Regular dressing and analgesia were not required.
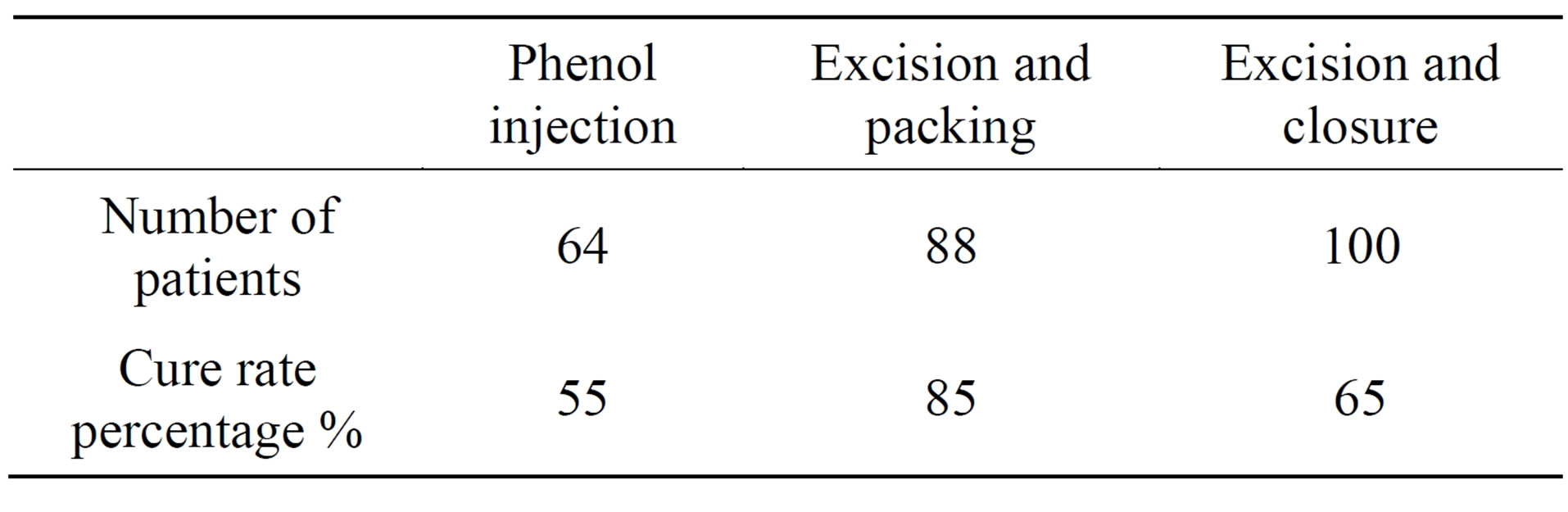
Table 1. Patients, procedures and cure rate.
Following excision of sinuses with packing, patients received daily dressing for 2 days at the hospital then discharged to do dressing at home. Thereafter, patients were reviewed at 2 - 4 weeks intervals until their wound healed. On the other hand, patients treated with excision and primary closure remained in hospital for one week, at least, with daily dressing. Outpatient follow-up was continued for a 2 - 4-week interval until the sinus healed. Follow-up was continued for 18 months to exclude or identify the recurrence.
3. RESULTS
An initial cure rate of 85% was obtained following excision with packing, 65% following excision with primary closure, and 55% following phenol injection (Table 1).
Analysis of cure rate relative to the number of sinus openings showed that for sinuses with one or two openings, there was no significant difference between excision and injection. Comparison of inpatient stay and time to healing revealed a significantly earlier discharge from hospital and a shorter time to heal following excision with primary closure and phenol injection (Table 2). During an average follow-up of 18 months (range 6 months to 4 years), recurred sinuses after initial healing occurred in 11 patients treated with excision and packing (12%), 15 patients treated by phenol injection (26.5%), and 23 patients treated by excision and primary closure (23%). Following 172 phenol injections in 64 patients, sterile abscesses developed in 5 patients (9%) and cellulitis in 1 patient (1.5%). There was no relationship between number of sinus openings and development of an abscess. The abscesses and related sinuses were all cured by surgical drainage while the cellulitis was settled with antibiotics treatment.
4. DISCUSSION
Pilonidal sinus can be a chronic and recurring condition which is sometimes difficult to cure. Many treatments have been reported but few provided long term good
results. The traditional method of in bloc excision and lay open of the sinuses result in hospital stay of 5 - 14 days, healing times of 6 - 10 weeks and recurrence rate of 8% - 21%, similar to the findings of this series [17,20,21]. Previous attempts to improve on these results by various methods of primary closure reduced the healing time to less than 2 weeks, but hospitalization remained almost the same between 7 to 10 days, and recurrence rate varied between 8% and 30% [22-25]. Such data appear favorable for the primary closure approach. However, the recurrence rate for this group was 23% compared with 12% for patients treated with excision and packing (Table 2).
Although the closure of the wound is more cosmetically acceptable for some patients and is associated with a shorter healing time-off work, this potential benefit is offset by the need of bed rest for up to 10 days in hospital coupled with a high risk of postoperative infection. Also, we must stress that when infection intervenes, the wound must be laid open and healing time becomes longer than in the case where the wound had been treated by secondary intentions in the first place [26].
Concerning the phenol injection, it is a closed technique that causes sclerosis and gradual closure of the pilonidal sinus [27]. There have been many reports on series of phenol injection of pilonidal sinuses. They described hospitalization of 2 - 3 days, healing within 3 - 6 weeks, return to work in 1 - 2 days and recurrence rate varying between 9% [28], 19% [29], and 40.5% [30], respectively.
However, the phenol method requires repeated injections, causes discomfort and pain for the patient, and until recently it was linked with relatively high recurrence rate (26.5% in our series and others). Also, we must not forget that the 9% incidence of sterile abscesses following injection was disappointing. We attributed this complication to the fact that the phenol is a necrotizing material [31]. These complications occurred mostly during the first period of our study and maybe be due to the lack of experience. Furthermore, care should be taken when working with this method to avoid any burns to the skin.
Another study of 41 patients using 2 - 3 applications of crystallized phenol [32] reported a recurrence rate of only 5% after 24 months without any complication. However, the lack of long-term follow-up and the small number of patients made this study not statistically significant and could not be considered generalizable.
Others advocated many other procedures such as skin flaps aiming to modify the anatomy of the pilonidal sinus natal cleft, considered to be responsible for the infection. They include skin flaps in the form of Z [30], rhomboid [33,34], Karydakis [33-37]. All these techniques, requiring careful execution, include the risk of cutaneous necrosis and a recurrence rate ranging from 0% to 28% [38] in studies monitored for almost three years. More time is needed to assess nearly all the recurrences. Ertan and co-workers suggested that such flap treatment must be reserved for patients with problematic pilonidal disease either in term of chronicity or failure to heal following excision [39]. Also, Ince suggested using sinosotomy technique and fibrin glue injection with good results [40,41]. While Kent reported the use of Matri Stem extracellular matrix xenograft in 9 cases which is not reliable due to the small number of cases [42]. Moreover, Smart found that using the ultrasound as guidance in excision of pilonidal sinus improve the results and make it simpler [43].
In brief, the authors prefer open excision and healing by secondary intention. Healing, in such cases, is usually relatively painless and leaving a linear, flexible scar. The percentage recurrence rate in our experience is 12%, which is considered convenient. It is less than in phenol injection (26.5%), or in excision with primary closure (23%) (Table 2).
5. CONCLUSIONS
Pilonidal sinus disease would still appear to be poorly understood both in terms of pathophysiology and the best treatment option. It is a complex condition that causes both discomfort and embarrassment to sufferers. Direct cost to the health care system and indirect cost through absence from work are high. This study shows that incision and drainage with curettage are recommended for treatment of pilonidal abscesses, while for pilonidal sinuses with one or two openings, phenol injection is an effective treatment. It has the advantage of a reduced requirement for analgesia and dressing, and a shorter inpatient stay and time to heal. We abandoned the excision and primary closure because of its high recurrence rate.
In fact, there is no ideal treatment until now. As suggested by Chintapatla, the choice of surgical approach depends on the surgeon’s familiarity with the procedure and the perceived results in terms of healing and recurrence rates [6].
Lastly, for patients, the choice would probably be the procedure that would be least inconvenient in terms of hospital stay, missed days of work, time to heal, recurrence rates and has the least impact on quality of life.