Utility and efficacy of navigation system use in interventional radiology ()
1. INTRODUCTION
Interventional radiology (IR) has been increasingly involved in minimally invasive diagnostic and therapeutic care of patients. The scope of practice for IR ranges from placement of catheters and needles to the treatment of tumors in patients using image guided technology [1]. The various techniques utilized by interventional radiologists provide symptomatic relief, treatment for certain cancers and increases patient survival [2]. Medical imaging in interventional radiology supports image guided therapy by assisting with pre-procedural planning, intraprocedural targeting, monitoring, control and post-procedure assessment [3]. Procedural execution depends on the skill set of the Interventional Radiologist. These physicians need to be skilled in interventional techniques and diagnostic interpretation of images while possessing a solid foundation of anatomy and patient care [4].
Interventional radiologists use sophisticated manual skills to manipulate devices in order to target specific tissue. There are a few navigation systems that are being used to enhance conventional IR by helping to guiding needles and guide-wires, in some cases using real time spatial feedback [1]. There are four main categories of guidance systems that can be used to assist IR: Optical system, Electromagnetic (EM) tracking, Cone Bean Computer Tomography (CBCT) and Magnetic Navigation. There are some indications for the use of each navigation systems and they possess both strengths but also drawbacks in their use.
It is important to summarize any current primary medical literature in regards to how interventional radiologists are utilizing navigation systems to treat patients across the globe. The purpose of this investigation is to examine some of the current medical literature available on navigation systems for interventional radiologic procedures. The relevance of this narrative review investigation will be to present an overall impression as to the state of navigation system use in interventional radiology.
2. MATERIALS AND METHODS
For this investigation, three health databases were selected: Pubmed, Embase (1996 to 2012 Week 31) and OVID Medline (1946 to September 2012). All databases were searched on September 10, 2012. The search terms used were “Interventional Radiology” and “Navigation System”. This combination was used to due to its broad scope to adequately represent the parameters for this investigation.
Studies were assessed if they were primary research that was related to the use of the common navigation systems in interventional radiology. All included studies were presented in English. Studies were excluded if they: did not pertain to navigation systems in interventional radiology, or were in a language other than English. Literature discussing navigation system use with surgical intervention as opposed to interventional radiologic procedure was also excluded. Additional reasons for exclusion included journal articles that were not accessible, literature presented as an abstract only, or literature discussing interventional cardiology. Studies identified were initially screened for inclusion or exclusion on the basis of the abstracts.
3. RESULTS
The appropriate studies were assessed for description of the advantages and drawbacks of the common navigation systems used in interventional radiology. Some consistent themes from these studies are presented in this section. For purposes of this report, the following navigation systems will be discussed: optical navigation devices, electromagnetic tracking, C arm based CBCT and Magnetic Navigation systems.
Optical navigation devices are able to continuously estimate positions of a moving target. They can be active or passive systems and have the ability to continuously estimate positions. Such devices are useful for three dimensional trajectory planning and needle placement [5]. However, there are several drawbacks to such devices. It is a bulky apparatus and has limited application in CT guided interventions. These devices also require a free line of sight between the cameras and optical markers [5]. Finally, while the needle hub can be optically tracked, it is difficult to effectively track additional regions of inserted needles [5].
Electromagnetic (EM) tracking functions on the basis of sensor coils with differential magnetic fields [1]. One of the major benefits of electromagnetic tracking of instruments in interventional radiology is real time display of position and orientation. It also allows interventional radiologists to guide needles toward a target within previously acquired three dimensional images to help avoid critical structures. Studies have found EM tracking able to improve operator confidence and increase accuracy of needle placement especially in lung biopsy and ablation procedures [6]. When other modalities present poor visualization of the target such as an ultrasound, EM tracking has been found more effective in such cases [6]. Repeated investigations have also demonstrated enhanced accuracy for procedures using EM tracking and reduced time to procedure. These investigated correlation increased accuracy with reduction in tracking error [6]. Finally, radiation doses have been found to be significantly lower in EM tracking compared with that used in CT guided procedures [6].
One drawback of electromagnetic tracking is the patient’s need to be immobilized for reduction of patient error due to respiratory motion and organ shift during the procedure. Operator time, automation of system setup, ease of use, integration with angiography system and cost effectiveness also remain issues with using electromagnetic tracking [7]. Furthermore, a trade off exists between positioning fiducial markers too close to the target, jeopardizing sterility and ensuring accuracy of the procedure. Finally, optimal field strength is imperative for the navigation system. EM tracking registration can be compromised by degradation of coil signal if the equipment is in the vicinity of metallic structures such as a CT gantry [6].
Moreover, C arm based CBCT when combined with image guided navigation is used for vertebroplasty, gastrostomy, stenting, biopsies and ablation procedures. The system has been found to increase technical success rates for procedures involving needle placement [6]. C arm based CBCT has two main factors that hinder more widespread adoption of its use. The first is concern for the patients’ accumulated radiation exposure [8]. Secondly, there is an assumption of immobility and rigidity of anatomy that is also seen in optical tracking. Additional limitations for CBCT include respiratory and patient motion, which can impair registration and therefore decrease accuracy.
Magnetic navigation systems consist of an externally generated magnetic field that controls and steers magnetically tipped medical equipment such as micro guidewire. The major advantage of this system is multi-directional magnetic orientation of the micro guidewire within vasculature [9,10]. This results in safer and more accurate intravascular navigation, reducing the chance of vessel dissection or perforation [9]. However, magnetic navigation systems have also been found to be easier, more accurate and faster to use in the hands of less experienced investigators while allowing for more predictable procedure times (Table 1) [9].
4. DISCUSSION
Interventional radiology is highly dependent on the precise accuracy of procedures such as needle, catheter and device placement. Navigation systems help guide interventional radiologists for where these devices need to be placed, using spatial feedback in relation to imaging data. Navigation systems are useful when entry angles are challenging or visibility of specific lesions is limited. Image guided interventional treatment requires a multidisciplinary approach to provide complete patient care. As technology changes, it is imperative to appreciate the new direction of treatment so patients have access to well trained expert interventional radiologists and imaging experts working in proper environments with the right equipment [11]. Previous investigations have demonstrated that interventional radiology has value in adults [12]. This investigation provides evidence of the integration of navigation systems in the discipline and the benefits and potential drawbacks.
Three general themes appear to consistently emerge within the literature in regards to navigation systems: procedural changes, monetary benefits and radiation exposure. Both advantages and drawbacks have been noted for integrating navigation systems into interventional radiologic procedures. The systems are able to help guide needles accurately toward a target along a preplanned trajectory while avoiding critical structures. This is safer for the patient and can avoid compromising the integrity of vessels through potential perforations. Some systems also allow for real time display of position and orientation. Furthermore, the use of navigation systems has also led to more predictable procedure times. This allows for more efficient scheduling of patients.
There are some drawbacks procedurally to the integration of navigation systems in interventional radiology. Some navigation systems have made procedures less dependant on operator experience and skills. A potentially troublesome trend may occur with the increasing development of IR technology and associated navigation systems. With standardization of integrated treatment plans, there will be a decrease in variability of practice patterns of the administered treatment. However, this may encourage less experienced operators to start delivering treatment. To ensure the highest standard of patient care, well trained expert interventional radiologists need to ensure standardization of the procedures. Training programs ensure a graduated system with residents in radiology learning fundamental skills particularly on simulators which can be helpful.
Respiratory motion and sterility are two additional issues consistently associated with navigation system use. Respiratory motion has the potential to compromise the integrity of the operator’s orientation within previously acquired three dimensional images. The other issue is that fiducial pads of the electro-magnetic system can get in the way and even compromise the sterility of a clinical procedure. A trade off therefore exists between potentially jeopardizing sterility and ensuring accuracy of the procedure The addition of new technology to the angio suite inevitably increases the overall cost of procedures. However in the long term, it is expected that any reduction in morbidity/mortality can reduce future hospital costs. Radiation dose is another drawback consistently noted in the studies, especially for CBCT. Studies have found exposure levels of the CBCT system lay between traditional CT and conventional radiograph [13]. Studies in the United States have found that most procedures can result in clinically significant radiation dose to the patient, even when performed by trained operators with use of dosereducing technology. As a result, it is important to ensure use of the most up-to-date equipment and document patient dose in the medical records.
The results of this investigation are as expected within the interventional radiology community. Such investigations can provide an overall understanding of the state of navigation system use. However, there are some limita-
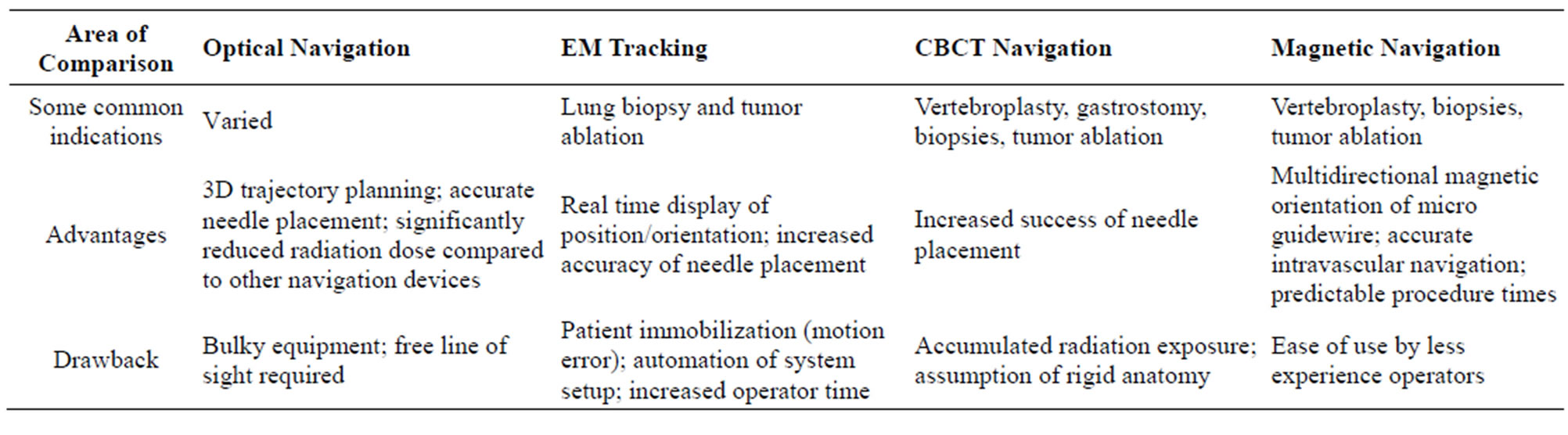
Table 1. Comparison of commonly used navigation systems.
tions to this study. This investigation attempted to summarize the broad features of navigation systems used in radiology, selecting the more commonly used devices. Also, while the major medical databases were consulted for this review, studies may have been missed. As only papers presented in English were assessed, it may be advantageous to investigate search engines in other languages to determine if any additional literature is present.
While there are many advantages to multi-detector, thin slice, high resolution CT scanning in assessing scaphoid fracture healing, there are some disadvantages. The first is that a higher radiation dose is needed than plain radiography. This drawback can be addressed by exposing only the area of interest to the radiation. Appropriate use of lead shielding, and having the patients stretch their arms above their head to limit the dose to the rest of the body can limit total body radiation exposure. The added limitation is the increased costs and reduced availability of CT scanners compared to plain radiography though is commonplace throughout hospitals in Canada and many countries worldwide. The increased cost of this investigation can be offset economically by definite early determination of fracture healing or lack of healing in follow up patients. For patients with definitive healing, as determine by the CT scan, morbidity can be reduced as they can return to work earlier by employing a short arm spica cast. For athletes in particular, CT assessment can allow for early onset exercises and decisions regarding avoidance of surgical intervention for the fracture.
The main strength of this pilot project lies in the novel approach of utilizing the 64 slice CT for definitive and unequivocal assessment of early scaphoid fracture healing by evaluating trabecular continuity as compared to the routine practice of follow up plain radiography. The main limitation of this investigation was the sample size. The intention of the investigators was to include 12 - 15 patients and analyze the results with chi-square and one way analysis of variance methods. Due to the small sample accrued, a meaningful statistical analysis could not be performed.
5. CONCLUSION
As navigation technologies evolve, their application to more complex procedures will better define their exact clinical roles and utilities. General themes appear to consistently emerge within the literature in regards to the advantages of navigation systems including benefits to interventional radiologic procedures such as increased patient safety, reduced procedure time and potential for reduction in costs. Increased radiation exposure, problems accounting for respiratory motion and sterility remain issues with the use of such systems.
Larger, national clinical trials with multiple sites and Interventional Radiologists studied over a longer period can provide greater insight into the efficacy of each system. With the potential to standardize treatment plans using navigation systems, more patients can have access to up-to-date technology for treatment. However, to ensure the highest standard of care, the use of navigation systems should be conducted by interventional radiologists only. With the improved accuracy, clinical utility and impact upon on patient outcomes, the use of navigation system in interventional radiology makes it vital to consistently review literature to under-stand trends and themes in the field.