Are There Early Clinical Factors to Decide Early Surgical Management for Secondary Chylothorax? A Review of 32 Cases ()
1. Introduction
Chylothorax occurs when the thoracic duct or its lymphatic tributaries become blocked or perforated or divided resulting in a chylous pleural effusion. In clinical practice, the most frequent cause of chylothorax is traumatic (post-surgical) and classified as secondary chylothorax. Spontaneous cause is called primary chylothorax and is caused by malignant lymph node diseases or congenital lymphatic diseases. Loss of chyle leads to nutritional deficiencies, dehydration, ionic perturbation and lymphocyte leaks thus increasing the vulnerability for infections and finally respiratory dysfunction by metabolic or mechanical mechanisms. Management of secondary chylothorax is a subject of controversy between medical or conservative treatment and surgical treatment.
As a general rule, surgical treatment is considered after failure of conservative treatment for several days. However, the period of medical treatment is not clearly identified and there is no evidence based medicine trials that have been founded for this management. Reviewing our series of patients treated for chylothorax, we want to identify early clinical variables allowing earlier surgical treatment rather than extended conservative medical treatment in case of secondary chylothorax.
2. Patients and Methods
A retrospective analysis of all patients treated between the years 2000 and 2010 for chylothorax in our thoracic surgery department, Haut-lêvèque Hospital, Bordeaux, France (a tertiary center of thoracic surgery) was performed. The patient files were coded on Excel (Microsoft) and analysed. The aim of the study was to identify early clinical variables allowing earlier surgical treatment rather than delayed surgery after time consuming medical conservative treatment. During the study period, management of chylothorax was performed with the following method: Diagnosis of chylothorax was firstly suspected in case of large amount of pleural leak or milky appearence of pleural effusion and confirmed by triglyceride level >110 mg/dl in doubted cases. When the pleural fluid triglyceride level is >110 mg/dL, there is <1% chance of it not being chylous, and pleural fluid with a triglyceride value of <50 mg/dL has no more than a 5% chance of being chylous. When the triglyceride level is between 55 and 110 mg/dL, a lipoprotein analysis is indicated to detect chylomicrons. In case of primary (spontaneous) chlothorax non-invasive assessment (thoracoabdominal CT scan, thoracocentesis, PET scan if needed) was first done. Later on, a video-assisted thoracoscopy was indicated for diagnostic purposes (allowing pleural and mediastinal exploration and biopsy) or for treatment by talc poudrage and drainage by two chest tubes. In case of secondary chylothorax a protocol of management was applied consisting of three steps. The first step was a conservative medical treatment with two subsequent managments. The first one consisted of thoracic drain if not done and low-fat oral diet in case of pleural fluid leakage less than 500 ml/day. The second was applied in case of pleural fluid leakeage of more than 500 ml/day and consisted of total bowel rest and parenteral nutrition with administration of a somatostatine analogue, during one week. Pleural fluid loss was compensated volume per volume with two-thirds 0.9% normal saline and one-third 5% albumine. Lipid soluble vitamins were added as well in association with one ampul of vitamin K per week. In the second step, lymphangiography was performed in certain cases. Lymphangiography was planned after the 8th day of conservative treatment if pleural fluid leakage per day is not decreased. Lymphangiography was considered as a diagnostic as well as a therapeutic procedure. The last step of treatment was realized more than 5 days after lymphangiography as the therapeutic effect of lymphangiography may be delayed. The last step was the surgical treatment. A blunt mediastinal or elective ligation of the thoracic duct was performed through right sided video-assisted thoracoscopy or right sided thoracotomy. A fat rich drink was routinely given an hour before the operation to enhance the visualization of the thoracic duct leak. The efficiency of the treatment applied was consisted by clinical assessment including vital signs at least three times daily, blood tests and chest X-rays every two days and the measurement of daily fluid loss graphically presented by a histogram. To check predisposing factors for early surgical treatment, patients were classified in two group: group 1, patients treated surgically after failure of medical conservative treatment (Table 2) and group 2, patients who were treated medically with successful results (Table 3).
3. Results
During the last ten years there were 32 patients diagnosed as having chylothorax, either admitted with chylothorax or chylothorax occurring after a planned surgery. There were 21 males (65.6%) and 11 females (34.4%) with a mean age of 55.7 years (range from 9 to 79 years).Twenty-two of the patients (68.75%) had chylothorax after a surgical intervention, seven patients (21.8%) had chylothorax due to medical causes and three patients (9.3%) after chest trauma. The causes of primary chylothorax were retroviral HIV infection in 2 cases, Paget disease in 1 case, cystic lymphangioma in 1 case, metastatic testicular carcinoma in 1 case, mediastinal fibrosis in 1 case, and associated with myasthenia gravis in one case. Chylothorax was resolved by medical treat-

Table 2. Patients treated surgically after the diagnosis of chylothorax.
ment in 1 case, by VATS with talcage in 4 cases and by thoracic duct ligation in 2 cases (mediastinal fibrosis and myasthenia associated case). Post traumatic chylothorax occurred in 3 cases. Leak cessation was obtained after medical treatment in 2 cases and duct ligation after lymphography was necessary in 1 case. Chylothorax occurred after a planned surgical intervention in 22 cases. Thoracic duct ligation was performed in 14 patients. The leak was stopped after surgery in 11 cases and surgery failed in 3 cases. The time spent before surgery varied between one week to one month in some cases. The average flow rate of leak for patients treated surgically was 1007 mL/day and for patients treated medically was 397 mL/day. Lymphography was performed in 9 cases, leading to leak cessation in 3 cases (33%) (Table 4).In our study post-operative complications associated with chylothorax include three cases of post-operative pneumopathy (9.3%), four cases of anemia (12.5%), two cases of atrial fibrillation (6.25%). Other complications include vocal cord paralysis, diaphragmatic paralysis, urinary
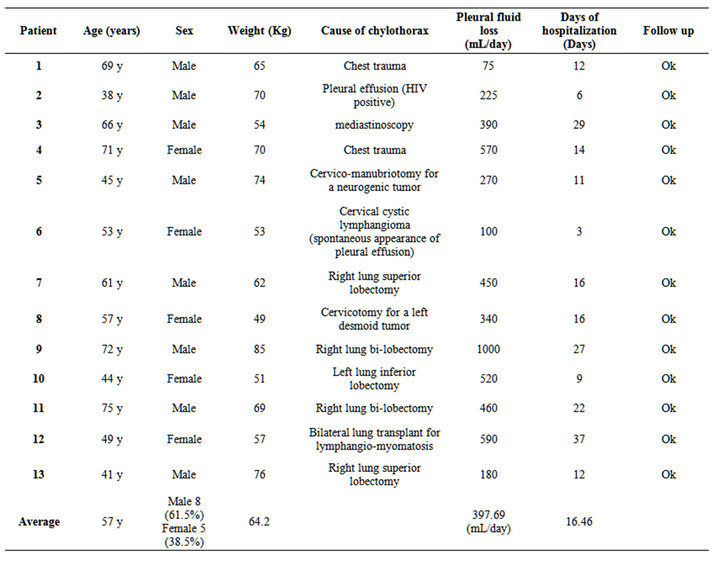
Table 3. Patients treated conservatively (medically) after the diagnosis of chylothorax.
infection and an edematous reaction at the level of a patients feet after lymphography (Table 5). Mean hospital stay was 36 days for group1 (patients treated surgically) and 16.46 days for group 2 (patients treated conservatively). We do not find significant difference between the two groups concerning patient characteristics except for the average of fluid loss that seems to be higher in the group of patients treated surgically (Figure 1).
4. Discussion
Our results are not so different than those reported in other series. According to our results, it seems that an earlier surgical treatment should be applied when the flow rate of the leakage is more than 500 ml/day after the 5th postoperative day.
Shimizu et al. [1] had reported that early surgical intervention may be indicated if chest tube drainage is more than 500 mL during the first 24 hours after complete oral intake cessation and total parenteral nutrition. Dugue et al. [2] have been reported the cut-off of 10 ml/kg at day 5 after the onset of chylothorax for the decision between conservative and surgical treatment in a series of esophageal resection. This strategy should be adapted to the type of surgery.
Esophageal resection is perhaps the most common iatrogenic cause of chylothorax, and an incidence of 4% has been noted in the literature [3].
Chylothorax arising after esophageal resection for carcinoma is more often due to the perforation of the thoracic duct itself and not one of its tributaries. In that case the flow rate of leakage is high (more than 500 ml/day) and medical treatment would fail and earlier surgical treatment should be applied.
In our experience, since the last 5 years we have been adopted new technology of tissue fusion (Ligasure) for esophageal resection. We have noticed reduction of operative time and incidence of chylothorax due to fusion of tissue fat pad in the infra-mediastinal space just above the diaphragm against the aorta.

Table 4. Patients who had lymphography after the diagnosis of chylothorax.
Prophylactic ligation of the thoracic duct during oesophageal surgery has been recommended by some surgeons to prevent chylous fistula [4]. Some advocate routine ligation of the thoracic duct, especially with tumors of the midoesophagus [5]. The incidence of post-oesophagectomy chylothorax reduced from 9 to 2.1% when elective ligation of the major thoracic duct was performed in a series of 255 patients [5].Concerning chylothorax after pleuropulmonary surgery we reported 8 cases of chylothorax after lobectomies for lung cancers with radical lymphadenectomy (2 left lobectomies and 6 right lobectomies). A conservative treatment was sufficient in 5 cases and surgery was necessary in 3 cases. Chylothorax occurring after lung cancer surgery is usually due to the perforation of one of the tributaries of thoracic duct. Conservative treatment with or without lymphangiography is usually sufficient except after pneumonectomy. In the literature there are a few cases of chylothorax after operations for diseases of the pleura. Endoscopic pleurolysis has frequently caused chylothorax.
Thoracoplasty, lobectomy and pneumonectomy are also common causes. Kuntz had reported some instances of chylothorax after segmental resection as well as one case after pulmonary decortication [6].
Chylothorax after cardiovascular operations was noted in three patients in our series. The first was after a coarctation of aorta operation, the patient had a thoracic duct ligation with no improvements and the chylothorax was stopped after restarting the conservative treatment after the failure of the operation. The second patient was a 9 year-old boy that had a cardiac operation due to a congenital anomaly, chylothorax was stopped few days after the performance of lymphangiography. The third case was after an operation of carotid subclavian bypass, for this patient chylothorax was stopped after ligation of the thoracic duct. Chylothorax has been reported after surgical treatment of the following cardiovascular malformations: tetralogy of Fallot [7-9], patent ductus arteriosus [10-12], tricuspid atresia [13], coarctation of the

Table 5. Other postoperative complications associated with chylothorax.
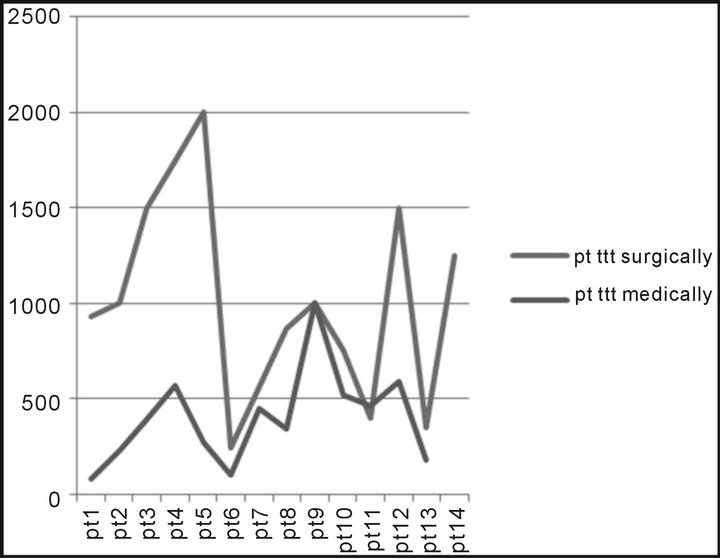
Figure 1. Comparison between the amount of pleural fluid loss for patients treated surgically and patients treated medically after the diagnosis of chylothorax.
aorta [14], and several complex malformations.
Chylothorax occurred in two cases after transplantation in our series. The first was after double lung transplantation for lymphangioleiomyomatosis in one case. Diagnosis of chylothorax was done on the 7th post-operative day and the leak was stopped after 7 days of medical treatment. Lymphangioleiomyomatosis is an uncommon progressive thoracic pathology in females of childbearing age. It results in nodular and diffuse interstitial proliferation of the smooth muscle in the lungs, lymph nodes, and thoracic duct. Two-thirds of the patients have chylous pleural effusion [15-17]. Chylothorax due to lymphangioleiomyomatosis was described in 6 cases of the 44 patients (13%) transplanted in the French experience (Reynaud-Gaubert) [18]. The second case was a chylothorax after heart-lung transplantation for sarcoidosis and pulmonary hypertension. This patient was also treated medicaly and chylothorax was stopped totally few days after performing lymphography. There are not much studies in the literature studing chylothorax after lung transplantation. Shitrit D [19] had noted that chylothorax can present late after lung transplantation and that conservative treatment should be considered in pateints with good nutritional status.
Chylothorax after mediastinal surgery had also reported in our study in one case after a diagnostic mediastinoscopy. Chylothorax was stopped after conservative treatment. Chylothorax occurs relatively often after operations for cysts and tumors of the mediastinum. There are frequent observations of chylothorax after the removal of mediastinal or cervicomediastinal lymphangioma. The statistical incidence of such a complication in this group is about 1.8 percent [20]. Gruwez [21] has reported a case of chylothorax after removal of a mediastinal goiter. Chylothorax after cervical surgery was observed in three cases in our study. The first was chylothorax after cervical dissection after the diagnosis of thyroid cancer. The second was after a cervical surgery for a desmoid tumor and the third for a neurogenic tumor. The first patient was treated by thoracic duct ligation, the second and the third patients were treated conservatively. Extensive neck dissections may give rise to postoperative chylothorax [22-24]. The possibility of injury to the thoracic duct is always present during operations for neoplasms of the cervical area, especially in operations necessitating removal of the jugular vein and the sternocleidomastoid muscle.
Thambo et al. [25] advocate lymphangiography as essential examination before surgical treatment of chylothorax for two reasons. First, it allows visualization of the thoracic duct anatomy as we should bear in mind that variation in the anatomy of the thoracic duct is common. Second, we believe in therapeutic role of lymphangiography by sclerotic effects of the thoracic duct vessels induced by ethiodized oil, a contrast agent used to opacify lymphatic network.
As the reason that surgical treatment should not be performed immediately after lymphography, but it should be performed around five days after lymphography.
This effect has been also reported by Matsumoto et al. [26] for various chyle leakages, in 8 of the 9 patients (89%) that Matsumoto included in his study, lymphatic leakage was stopped after lymphangiography and surgical re-intervention was avoided. However, lymphangiography is a time consuming assessment requiring great skill and patience, and is performing by only one radiologist in our radiology department. That explains why in our series lymphangiography was performed in only 9 cases of the 22 post-operative cases depending on availability of the radiologist. It is a safe assessment and more useful than lymphoscintigraphy.
5. Conclusion
Although many cases of chylothorax can be cured with a conservative managment, early surgical intervention may be indicated if chest tube drainage is more than 500 mL during the first 24 hours after complete oral intake cessation and total parenteral nutrition.