Factors associated with psychological distress of Public Health Nurse in Kagawa prefecture, Japan: A pilot study ()
1. INTRODUCTION
About 14% of the global disease burden has been attributed to mental illness, mostly due to the chronically disabling nature of depression and other common mental disorders [1]. Mental health has become public health challenge in Japan. For example, over 30 thousand subjects suicide in a year for over 10 years [2].
Recently, the demand for nurses has been increasing in various areas because of a medical reform bill and government amendments to the medical service payment structure in Japan. In addition, public health nurse, who works for community and company for public health in Japan, has become also more required. In some literatures, the psychological distress of nurses in hospitals has reported [3-7]. However, the evaluation of psychological distress of public health nurses in Japan still remains to be investigated.
Therefore, we evaluated the psychological distress of public health nurses by using the K6, the scale of psychological distress, in Kagawa prefecture, Japan and its relation to considerable factors in this cross-sectional investigation study.
2. SUBJECTS AND METHODS
2.1. Subjects
We used data of 271 public health nurses among 419 public health nurses in Kagawa prefecture, Japan, who met the following criteria; 1) they had completely answered the questionnaires and 2) they provided informed consent. Therefore, we analyzed 256 (61.1%) public health nurses (1 man and 255 women), aged 42.5 ± 11.2 years. Ethical approval for the study was obtained from the Ethical Committee of Faculty of Medicine, Kagawa University, Japan.
2.2. Psychological Distress
The K6 was used as and indicator of psychological distress [8,9]. The 6 questions were as follows: “Over the last month, how often did you feel: 1) nervous; 2) hopeless; 3) restless or fidgety; 4) so sad that nothing could cheer you up; 5) that every thing was an effort; 6) worthless?” (Table 1). Participants were asked to respond by choosing “all of the time” (4 points), “most of the time” (3 points), “some of the time” (2 points), “a little of the time” (1 point), and “none of the time” (0 points). Therefore, total point score ranged from 0 to 24. The K6 has been developed using modern psychometric theory and has been shown to be superior to some existing scales in brevity and psychometric properties [8-10]. The Japanese version of the K6 has been recently developed, using the standard back-translation method, and has been validated [11]. As suggested by Kessler et al. [10], we classified participants with scores of 13 points or more as having psychological distress.
2.3. Measurement of Variables
The questionnaires for public health nurses consisted of the following details in sequence: age, sex, experience duration as public health nurses. In addition, we evaluated the consciousness of suicide, anxiety of preventing suicide and cooperation with specialist in their daily work.
2.4. Statistical Analysis
Data are expressed as mean ± standard deviation (SD) values. A statistical analysis was performed using ANOVA and Scheffe’s F test. Simple correlation analysis was performed as well to test for the significance of the linear relationship among continuous variables, where p < 0.05 was considered to be statistically significant.
3. RESULTS
A total of 15 public health nurses (5.9%) was defined as psychological distress. We evaluated the relationship between the K6 score and age (Figure 1), experience duration as public health nurse (Figure 2). Clear relationships between the K6 score and age (r = –0.175, p = 0.005), and between the K6 score and experience duration as public health nurse (r = –0.133, p = 0.034) were not noted in this study.

Table 1. The K6 included 6 questions was a scale of psychological distress.

Figure 1. Relationship between the K6 score and age in public health nurse in Kagawa prefecture, Japan.

Figure 2. Relationship between the K6 score and experience duration as public health nurse in Kagawa prefecture, Japan.
In addition, we evaluated the factors i.e. consciousness of suicide, anxiety of preventing suicide and cooperation with specialist (Table 2). The K6 score in subjects with anxiety of preventing suicide was significantly higher than that without (p = 0.002). The K6 score in subjects without cooperation with specialist was also higher than that in subjects with that, but not at a significant level (p = 0.239). However, significant differences were not noted between subjects with and without consciousness of suicide (p = 0.772).
Finally, the K6 score in subjects who feel their own mental status was excellent was also lower than that in subjects feeling bad or poor, by one way ANOVA (Figure 3).
4. DISCUSSION
We firstly evaluated the psychological distress using the
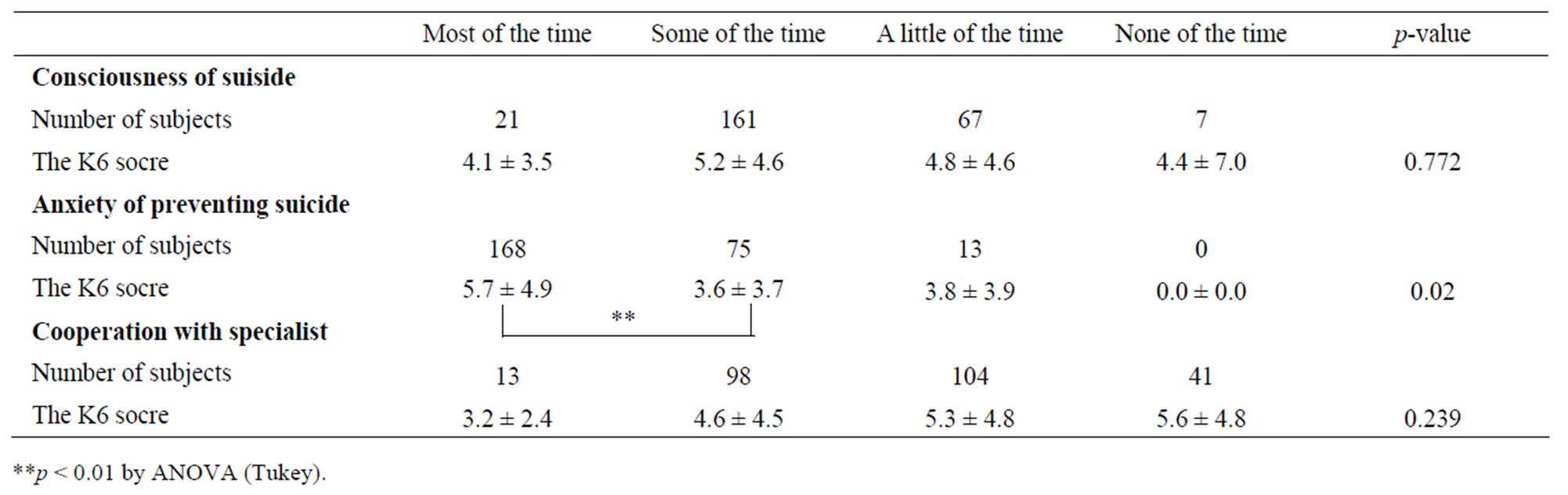
Table 2. Relation between the K6 score and considerable factors in public health nurse.
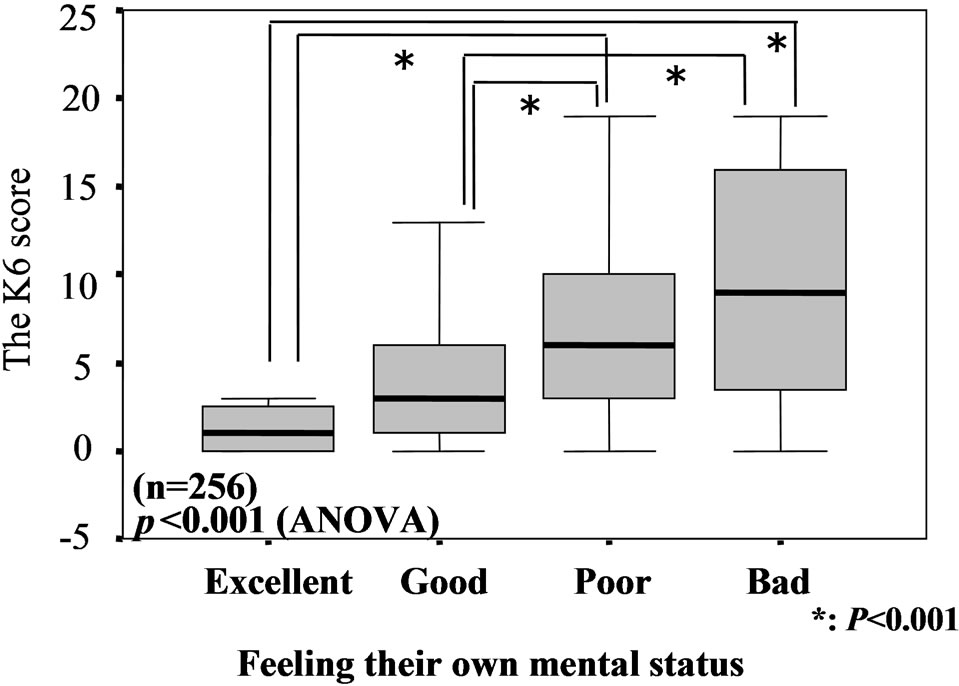
Figure 3. Relationship between the K6 score and feelings of their own mental status in public health nurse in Kagawa prefecture, Japan.
K6 in public health nurses in Kagawa prefecture, Japan.
According to the link between psychological distress and nurses in hospitals, Katayama has reported that the aspects of “suppressed expression”, “deep adjustment”, and “surface adjustment” of emotional labor seem to be the major occupational stressors for nurses [3]. Tei-Tominaga et al. showed that they obtained 301 newly graduated nurses and found that psychological distress was important predictor of intentions to leave in a longitudinal analysis [4]. Ishihara et al. also reported that the levels of urinaly 8-hydroxydeosyguanosine (8-OHdG), which reflects oxidative DNA injuries, in subjects with shift work was higher than that in subjects with part time work [6]. Munakata et al. also showed that psychological disturbances after night work were associated with altered cardiovascular and endocrine responses in healthy nurses [7]. In this study, we evaluated the psychological distress using the K6 in public health nurses in Kagawa prefecture, Japan. Consciousness of suicide and anxiety of preventing suicide in their daily work might be associated with psychological distress in public health nurses in Kagawa prefecture, Japan. Therefore, it seems reasonable to suggest that simply supporting in public health nurses in mental health and suicide is required in Kagawa prefecture, Japan.
In some literatures, psychological distress by using the K6 has been reported. Kuriyama et al. reported that they evaluated psychological distress of 43,716 communitydwelling people aged 40 years or older living in Japan [12]. Inoue et al. showed that part time workers in men and temporary/contract workers in women were associated with poor mental health in a total of 9461 men and 7777 women employees. No clear relation in mental health was noted in company size or occupation [13]. Subjective social status seems to be a stronger predictor of psychological distress among both men and women in the Japanese community than traditional socioeconomic status [14]. However, there was no report of psychological distress of public health nurse in Japan. In this study, by using the K6, we evaluated the psychological distress of public health nurse in Kagawa prefecture, Japan. A total of 15 public health nurses (5.9%) was defined as psychological distress. The rate of psychological distress was similar to that previous report [12]. However, some factors in their daily work might be associated with their psychological distress. This reference and pilot data obtained from this study will be useful for preventing psychological distress in public health nurses in Japan.
Potential limitations still remain in this study. First, our study was a cross sectional and not a longitudinal study. Second, 256 public health nurses in our study voluntarily underwent measurement: they were therefore more likely to be health-conscious compared with the average public health nurses. To show this, further prospective studies are needed in the Japanese.
NOTES