ECG and Echocardiography Findings: A Comparative Study between Sportive and Sedentary Female Patients (Bamako, Mali) ()
1. Introduction
Physical activity medically and epidemiologically refers to activities that lead to a substantial increase in oxygen consumption [1] .
Regular sports practice has undeniable beneficial effects for health in general and especially for the cardiovascular system. However, regular, intense and prolonged physical activity, although beneficial, leads to clinical, electrical, morphological and functional changes in the cardiovascular system. These cardiovascular changes seen in high-level athletes are known as “athlete’s hearts” and are benign [2] .
It is also true that the risk of a cardiovascular event is temporarily increased during an intense sport practice that may reveal an unknown heart disease. The causes of non-traumatic sudden death in sports fields are 85% - 90% of cases of cardiovascular origin and are secondary to cardiac arrhythmias [3] [4] [5] [6] . Thus recommendations have been formulated for sporting practice [6] [7] .
Data on athletes in general and especially footballers are rare for African countries, even sport practice and competition is growing and more and more professionalized. To our knowledge, in Mali, there are no published studies on athletes, even medical theses have dealt with the thema. There is no comparative electrocardiographic and echocardiographic data in trained footballers women and sedentary women leading us to perform this study aiming to present electrocardiographic and echocardiographic features in high-level athletes and sedentary women in Bamako.
2. Materials and Methods
Data derived from a cross-sectional study performed in Bamako from April 2015 to March 2016 among high-level footballers and a group of untrained women.
Included were all aged than 14 years consenting female subjects either as sportswomen (footballer) or as sedentary. Footballer was recruited in training centers in and sedentary randomly selected in high schools with the approval of school authorities. Following definitions were used:
· As sportwomen were considered, a female subject with at least 10 hours weekly training and for at least one year.
· As sedentary was considered, a female with no regular physical activity
Each subject received after interrogation and clinical examination, 12-leads electrocardiogram recorded using CONTEC ECG300G and an echocardiography performed by cardiologists with an ATL 5000 echocardiography machine. Each electrocardiographic record was analyzed by cardiologists according to the Seattle 2013 criteria as well echocardiograms.
A formulary was used to collect data including socio-demographic, physical examination, ECG record and echocardiogram.
Data were inserted in Microsoft Excel and analyzed with IBM SPSS. Chi Square and Fisher statistical tests were used to compare our results. The significance level was p < 0.05.
3. Results
Our sample included 43 female subjects of whom 51% were sedentary. Mean age of footballers was higher than that of sedentary women (P < 0.0001). Most footballers were in age group 20 - 24 whereas sedentary women merely in 15 - 19 years age group (Diagram 1).
Weight, height and body mass index were significantly higher for footballers than for sedentary women with 56.52 Kg, 165.67 cm and 20.61 Kg/m2 versus respectively 50.05 Kg, 161.36 cm and 19.18 Kg/m2. The corresponding p values were respectively 0.003, 0.036 and 0.035 (Diagram 2). One subject had hypertension.
Mean heart rate (HR) and PR duration were significantly different with HR lower for footballer (65.71 versus 82.68) but higher for PR duration (180 versus 156.36). The p values were respectively < 0.0001 and 0.010 (Table 1).
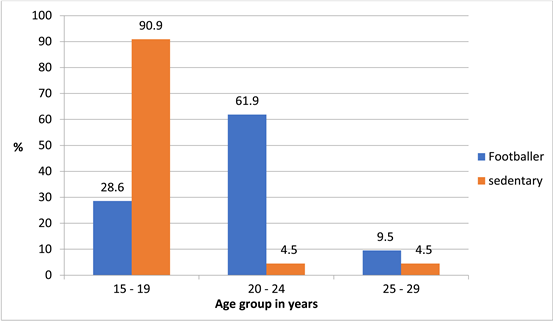
Diagram 1. Age group distribution in the sample of 43 footballers and sedentary female subjects with proportions in percent and p-value.
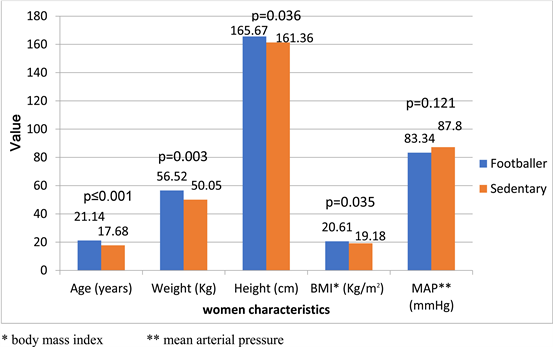
Diagram 2. Distribution of clinical characteristics of 43 footballers and sedentary female subjects with proportions given in percent.
Bradycardia was more common among footballer (28.6%) versus 0.9% among sedentary women in opposition to tachycardia which was found in 18.2 of sedentary women and not at all among sportswomen (Table 2). There was no significant difference of wide PR, corrected QT nach Bazett and ST elevation with p respectively of 0.522, 0.432 and 0.631 (Table 2).
Means for aortic, left atrium and left ventricle diameters were higher for the footballers with 26.81 mm, 32.14 mm and 47.33 mm versus 24.36, 28.32 and 42.14 for the sedentary women. These differences reached statistical significance with p values of 0.001, 0.010 and 0.018. There was no statistically significant difference in mean indexed left ventricle diameter, ejection fraction (Table 1).
![]()
Table 1. Means for ECG and echocardiography parameters.
*corrected QT based on Bazett formula +: left atrium, ++: left ventricle diameter, +++: left ventricle indexed on body surface, EFT: ejection fraction Teichholz.
![]()
Table 2. ECG and Echocardiography abnormalities in the sample of 43 female subjects.
LV* indexed on body surface.
Left ventricular hypertrophy was found in 28.6% of athletes compared to 04.5% of sedentary women (p = 0.033) and was more important in the age range 25 to 29 years by footballers (Table 2).
4. Discussion
Few studies have concerned female footballers in general [8] - [12] , and even fewer have focused on electric and echocardiographic changes compared to sedentary women.
Our study of 43 women (21 footballers and 22 sedentary) in Bamako included highlights the difficulty of recruiting women athletes for various reasons as mentioned by Reimers [8] . In our context as in other countries, sport and especially football is widely practiced by men and for many women sport and football is considered as an activity for men. Even if changes are observed, there is an under-representation of female in sport activity as pointed out by Mounkoro and Tiela [11] [13] .
The mean age of women footballer was higher than that of sedentary women. Even practiced by a few numbers of female subjects, football concerned those around 20 years and more.
The significant increase in weight and body mass index among women footballer could be explained by the effect of sport on body through the development of muscle mass dependant on the increase in the limits of normal weight and BMI. No case of obesity was found in our study.
5. Analysis of the Electrocardiogram
5.1. Heart Rate
Bradycardia was significantly noted among footballers (28.6%), opposed to tachycardia among sedentary (18.2%) with p = 0.006. This could be due to the effect of training on heart rate through vagal hypertonia [14] . This high frequency of bradycardia was emphasized by some Papadakis and Sheikh in two studies comparing black and white athletes [15] [16] where sinus bradycardia occurred in 47.1% and 41.9% of black athletes, respectively, compared to 60.7% and 58.0% in white athletes. These rates were higher than ours and this difference could be explained by the sex of the subjects on the one hand and by the nature of the practiced sport.
5.2. PR Duration
Sport can induce an AV-block I at rest, which is a priori, considered as benign and sign of a decrease in sympathetic tone and an increase in parasympathetic tone. It could exist before the sport practice according to Brion [12] .
In the sample 02 footballers a prolonged PR versus 1 sedentary subject without any statistical significance as noted by the p-value of 0.199. This phenomenon is widely reported by several authors: Lahardy [17] reported 7 subjects with a 1st degree AV-Block versus one 2nd degree AVB; Sheikh [16] reported 8.9% 1st degree AV-Block among black athletes compared to 2.5% for white athletes and Papadakis [15] reported 11.2% of 1st degree among black athletes versus 3.6% among whites. Brion [12] reported 3% 1st AV-Block among black sportsmen. In our context abnormalities of the PR duration was found in 1.9% in Mounkoro study [11] .
5.3. QRS Duration
In our sample, the mean duration of QRS was 80 ms. No subject had a QRS enlargement. There was no significant difference between the duration of QRS in sportswomen and the sedentary (P = 0.469). This result was different from that of Papadakis [15] who noted a proportion of 11.2% of incomplete right bundle block. In Malian context, the QRS duration was normal in 95.3% and 90% respectively in the studies of Mounkoro [11] and Tiela [13] . Our difference could be due to the small size of the sample.
5.4. The Sokolow Index
Left ventricle hypertrophy (LVH) according to the Sokolow-Lyon index is more common among athletes. We didn’t find any case of LVH, probably because of the small sample, whereas Rawlins [18] found it in 8.2% among sportswoman.
5.5. Corrected QT Based on Bazett Formula
Athletes have often bradycardia which leads to a significant lengthening of the QT interval. [19] . This corrected QT prolongation not exceeding 500 ms is usually attributed either to a delay in repolarization due to an increase in left ventricular mass in athletes or to a maladaptation of Bazett’s formula to low heart rates [12] .
In our sample, Bazett cQT was not significantly different between the two groups.
5.6. ST Modifications
Early repolarization was observed in 04 sports against 03 sedentary. This particular aspect of the ST segment is frequently observed in black subjects and even more so in black female subjects. These abnormalities of repolarization have been widely described by Papadakis and Sheikh in black athletes [15] [16] . These disorders of repolarization were essentially found in the anterior location in our study. There was no significant difference between sedentary and sportswomen (P = 0.632).
5.7. The Location of the Negative T Wave
In our sample, the negative T wave accounted for 88.4% in the anterior location. Papadakis [15] and Sheikh [16] reported lower rates among black athletes with respectively 12.7% and 22.8%.
6. Analysis of Transthoracic Doppler Echocardiography
As pointed out by Boisseau [19] , there are few heart studies among female subjects unlike male subjects, which explain the scarcity of data in this area.
6.1. Indexed Diameter of the Left Ventricle
This was the most frequently found abnormality with 51.2%. The mean left ventricular diameter indexed to the body surface was 28.65 mm/m2. The diameter of the left ventricle was larger in women athletes (47.33 mm) than in sedentary women (42.14 mm) with P = 0.018. This finding had been made by other authors including Papadakis and Sheikh [15] [16] . Training will increase the volume of the left ventricular cavity in athletes as reported by Abergel [20] . Pellicia [21] found a mean left ventricular diameter at 48 mm in female athletes. This rate is in agreement with our data. Extreme values of 70 mm have already been reported by Huston and Abergel [22] in other studies, particularly by world-class cyclists.
6.2. Left Ventricle (LV) Mass
LV mass was abnormal in 28.6% (n = 6) of women athletes compared to 04.5% (n = 1) of sedentary women. This increase in body surface index weight is probably related to the physiological dilatation of the ventricle. This finding is consistent with the results of many authors, especially since this increase is not accompanied by a parietal thickening [23] [24] . The LV mass is always increased in high-level athletes: compared to control groups, there is an increase in indexed LV mass from 50% to 100% [23] [24] [25] . The data of these authors are similar to ours and this increase is significant in our study with p = 0.033.
6.3. Ejection Fraction (Teichholz)
The LV function was good in all subjects of our sample, which is not surprising for sportswomen. Even for professional athlete athletes, LV ejection fraction is normal [1] [2] [9]
In general, resting values are comparable to those of non-athletic healthy subjects [20] . In the study, only two sports subjects had a slightly decreased ejection fraction, i.e. 9.5%, with no significant difference with sedentary subjects (P = 0.138). This small decrease is compensated for by the dilation of the left ventricle and also the bradycardia at the origin of a greater efficiency of the left ventricle.
7. Conclusion
Bradycardia, left ventricle hypertrophy and dilatation were found more in sportswomen. These changes acquired through physical training are aspects of cardiac adaptation that we found in our sample. Other aspects were not found probably due to the small size of the sample.