Assessment of Hearing Status by Pure Tone Audiogram—An Institutional Study ()
1. Introduction
Hearing is an important and essential sense for verbal communication, language skills and personality development. Hearing loss is the second most common disability in India after the loco motor disability. More than 40 dB hearing impairment in patients above 15 years and more than 30 dB hearing impairment in patients below 14 years in the better ear are considered as hearing disability.
Hearing loss is classified as:
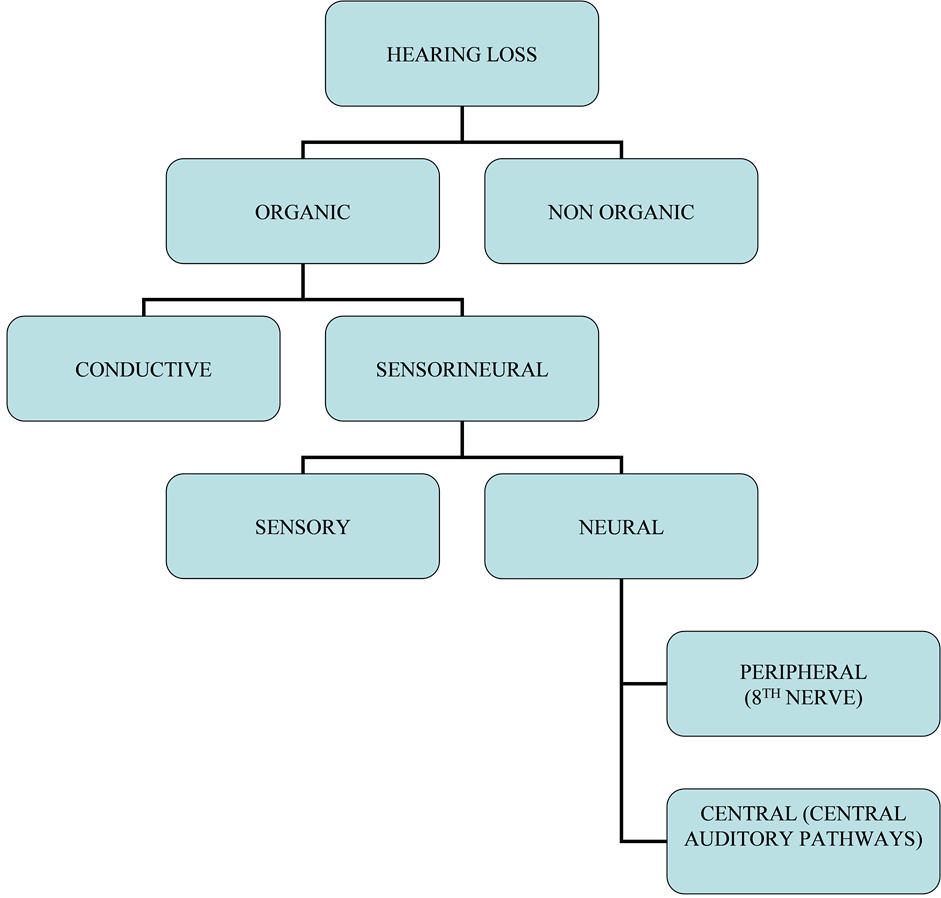
Conductive Hearing Loss: Any disease process which interferes with the conduction of sound to reach cochlea causes conductive hearing loss. The lesion may lie in the external ear, tympanic membrane, middle ear or ossicles up to stapedio-vestibular joint.
Sensorineural Hearing Loss: Results from lesions of the cochlea, 8th nerve or central auditory pathways. It may be present at birth (congenital) or start later in life (acquired).
According to WHO census, around 360 million have hearing disability and the majorities are adults (91%) and children are only 9%. Prevalence of hearing loss is more in the age group above 65 years [1] . Our study shows that age group of 50 years and above are involved more in number than other age groups.
National Institute on Deafness and other Communication Disorders (NIDCD) states that 15% of the population is having hearing loss due to loud noise in the working place or due to prolonged use of mobile phones [2] . Prolonged use of mobile phones for more than 30 minutes can cause 10 dB transient hearing loss [3] . As per the available information, about 6.3% of the Indian population is suffering from hearing impairment. Among these, the rural populations are more commonly affected than the urban population [4] . Hearing loss in children may affect their education due to the defective development of perceptual and linguistic abilities, because of reduced aural input [5] . Most common cause for hearing loss in children is serous otitis media or glue ear.
Sudden Sensorineural Hearing Loss (SSNHL) is defined as greater than 30 dB hearing impairment, over at least three contiguous frequencies, occurring over a period of 72 hours or less. Males are more commonly involved than females and the vulnerable age group is around 45 - 49 years. Presbyacusis or age related hearing loss is a slowly progressing one and involves both ears equally. Initially it affects the higher frequencies and later affects the lower frequencies also. The first sign is inability to understand the speech in noisy surrounding.
In pure tone audiogram, the tested frequency ranges from 250 Hz to 8000 Hz, and hearing level from −10 dB to 120 dB. This test is both qualitative and quantitative (Type and Severity of hearing loss). The degree of deafness is classified based on WHO (1980) classification with reference to ISO: R.389-1970 (International Calibration of Audiometers) as follows:
Normal Hearing 0 - 25 dB
Mild Hearing Impairment 26 - 40 dB
Moderate Hearing Impairment 41 - 55 dB
Moderately Severe Hearing Impairment 56 - 70 dB
Severe Hearing Impairment 71 - 90 dB
Profound Hearing Impairment >90 dB
Aims and Objectives
The aims and objectives are to assess the hearing level, the degree and type of deafness in patients attending the outpatient department.
2. Materials and Methods
This is a prospective study conducted in our institution. Patients who attended the Department of Otorhinolaryngology and Head and Neck Surgery OPD from Jan-Dec 2014 (about 1575 patients) were taken for study. The age of patients varied from 10 to 70 years. All patients were subjected to pure tone audiometry (MAICA-MA52) after an otorhinolaryngeal examination. Both air conduction and bone conduction were measured with Hughson Westlake technique modified by Carhart & Jerger and plotted in graph. Most paediatric patients were subjected to tympanogram also. Male: Female ratio, age distribution, degree of deafness and type of deafness were evaluated.
3. Results and Analysis
Our study shows that 64% of males and 34% of females are involved. Among males, the 40 - 59 years age group is more commonly affected, this correlates with WHO data. Among females, the 20 - 39 years age group is more commonly affected (Table 1). Our study shows that 40 - 59 years age group is more commonly involved (38%), 20 - 39 years age group constitutes 30%, above 60 years constitutes 20% and the rest 12% is 10 - 19 years group.
This study reveals that 42% are suffering from sensorineural hearing impairment, 15% from conductive type, 14% shows mixed type and the rest 28% have normal hearing (Table 2).
In this study, about 29% have mild degree of deafness, 26% have moderate degree, 11% have severe degree, 6% suffer from profound to total deafness and the remaining 28% have normal hearing. Moderate degree of deafness is common above 40 years. In our study, profound and total deafness is evenly distributed in all age groups (Table 3).
4. Discussion
In our study the majority of patients belong to the male sex (64%). Among the males, 4th and 5th decades are more vulnerable age groups. Around 28% of the cases are unilateral. Pure tone thresholds in females are lower at higher frequencies compared to males, suggesting that aging process begins earlier in men. Conductive hearing loss is more common in younger individuals and as the age advances sensorineural hearing loss predominates. The majority of subjects with hearing loss belong to working age group. This is probably due to occupational noise exposure, stress and trauma. Subjects working in industries are more vulnerable for noise induced hearing loss.
Tucker has argued that hearing is an ability that may be apprehended, thus screening for hearing at school entry level, especially for suspected unilateral mild to moderate hearing loss should be considered [5] . Robinovich
![]()
Table 1. Sex distribution in different age groups.
![]()
Table 2. Age wise distribution of type of hearing loss.
![]()
Table 3. Age wise distribution of degree of hearing loss.
has stated that early identification of hearing loss and adequate corrective measures help in better speech, language, social, psychological and educational development and a more satisfactory outcome [6] .
More recently Dr. Frank Lin and his colleagues at Johns Hopkins University found a strong relationship between degree of hearing loss and risk of developing Dementia. Patients with mild degree have 2 times, moderate degree 3 times and severe degree has 5 times the risk than normal hearing individuals [7] . Hearing loss is an invisible handicap. Although it occurs in an increasing prevalence with age, hearing loss is often ignored during the diagnosis and treatment of cognitive and memory disorders in elderly patients.
Sudden sensorineural hearing loss is nowadays increasing in incidence. The causes may be infection, circulatory problems, meniere’s disease, neoplasms, trauma, metabolic disorders, immunologic disorders or idiopathic. So in all cases of this type of hearing loss proper investigation regarding the etiology is very important. We did all relevant investigations and in many cases we found that viral infection is the culprit and some cases are idiopathic. The treatment includes systemic or oral steroids, hyperbaric oxygen therapy, antiviral drugs, vasodilators and chemorheologic agents. Most of the sudden sensorineural hearing loss patients presented with symptoms similar to eustachian tube catarrh. Because of this most patients presented with total hearing loss at the time of consultation. So in all cases of hard of hearing, audiological evaluation is mandatory and we have to do that at the first visit itself. Among all, pure tone audiometry is the most reliable, easy and cost effective method when compared to others.
Morbidity due to hearing loss in paediatric age group is inversely proportional to the literacy of parents. Most common causes for deafness in paediatric age group are Otitis Media with Effusion (OME), eustachian tube dysfunction, chronic suppurative otitis media and acute otitis media. For all these cases infection plays a major role, and it is more prevalent in low socioeconomic status and families with illiteracy. Infection is the most common cause for hearing loss in developing countries according to WHO data [8] .
Tharwat and his colleagues, 1998, and Arts and others, 2002, stated that cochlear implants are needed for those patients with bilateral profound to total hearing loss who could not be benefitted with formal hearing aids and it is recommended especially in the younger age group [9] .
In our study, most of the paediatric age group patients suffered from conductive type of deafness. Most common etiology for this is Otitis Media with Effusion. Pneumatic otoscopy is the diagnostic tool for this OME, but Tympanometry is the gold standard. Hence all those patients were subjected to impedence audiometry. Most of them were found to have Glue ear and received treatment and recovered completely. Treatment includes both medical and surgical management in the form of myringotomy and grommet insertion. Conductive type of hearing loss in adults are due to chronic suppurative otitis media and these are managed by mastoidectomy, if there is no improvement after the clearance of septic foci and medical management.
Auditory Neuropathy Spectrum Disorder (ANSD) is a type of hearing disorder in which the pure tone audiogram shows near normal hearing to profound hearing loss. But these groups can be confirmed by other tests, such as Oto Acoustic Emission (OAE) and Cochlear Microphonics (CM) which shows normal response and the Auditory Brain-Stem Response (ABSR) which shows abnormal or absent response. The site of lesion for this type of disorder is probably the inner hair cells of cochlea, spiral ganglia and the auditory nerve. Hyperbilirubinemia, anoxia/hypoxia, prenatal/neonatal infections, immune disorders are possible risk factors for this disorder [10] . So a detailed evaluation of antenatal, natal and postnatal history is important to identify this spectrum of disorders.
Noise induced hearing loss caused by exposure to recreational and occupational noise results in devastating disability that is virtually 100 percent preventable. This is the second most common form of sensorineural hearing deficit, after presbyacusis. Here the excessive sounds damage the stereocilia of the outer hair cells, therefore it is due to excessive wear and tear of delicate inner ear structures. Concurrent exposure to ototoxic drugs plays an additive effect. In olden days it was called as Boilermaker’s disease. This type of hearing problems can be prevented by using earplugs or earmuffs. Noise induced hearing loss begins at higher frequencies (3000 - 6000 Hz) and produce bilateral symmetrical loss [11] .
5. Conclusions
Pure tone audiometry is a simple and accurate method for the diagnosis of hearing impairment. Deafness prevention can be done only by mutual cooperation of both medical and non medical personnel. Majority of patients belong to the working age group. Hence early identification with timely intervention can reduce the morbidity of deafness in this age group which in turn helps to improve the productivity of the nation.
Hearing impairment leads to social isolation in elderly persons. An early and adequate diagnosis has an important role in adapting sound amplification devices and rehabilitation procedures for auditory function in elderly. In paediatric age groups, cochlear implant is possible if deafness is identified in the early stage. This in turn helps to improve their language and social and personality skills.