1. Introduction
Standards regarding Emergency Medical Service (EMS) use of lights and siren in emergency medical transport have recommended that their use in emergency medical vehicle (EMV) transport should be reserved for situations where improved response time will improve the patient’s chance for survival or quality of life [1]. While using lights and siren during emergency response has been shown to improve response time, the use of lights and siren has also been thought to cause an increased number of crashes involving vehicles near the ambulance [2]. The crash risk associated with this “wake effect” may outweigh the benefit associated with a slightly reduced response time. The goal of faster response time is to increase survivability in patients requiring time-critical medical attention. However, patient illnesses requiring timecritical response are relatively rare, and a limited list of illnesses has been examined in studies confirming increased survivability rates. The specific patient illnesses currently associated with EMV use of lights and siren deserve further study to determine whether the time saved in lights and siren travel is enough to justify their use in emergency response, or if the list of illnesses requiring lights and siren transport needs to be expanded.
1.1. Transportation Mode in Ambulances
Calls for assistance from EMS care providers are divided into three main categories: emergency, urgent, and scheduled transports. An emergency transport involves a request for immediate assistance that requires use of lights and siren. An urgent transport is performed following a request for immediate assistance that does not require lights and sirens. Scheduled transports are previously arranged appointments to transport a patient, such as moving an elderly patient to a new care facility, that do not require use of lights or sirens.
1.2. Transportation Mode and Response Time
One metric commonly used to evaluate EMS groups on their quality of provided care is the elapsed time from when a call is received until arrival on-scene. A new criterion that many EMS agencies are being encouraged by their managers to meet is a response time of eight minutes or less—a standard developed around a study of cardiac arrest patient outcomes in relation to response time [3]. Subsequent studies have not all agreed on the appropriateness of this eight-minute goal. Researchers supporting a reduction in response time have said that reducing this response time to five minutes would raise survival rates for cardiac arrest patients from 8 percent to 10 percent [4]. By contrast, Pons and Markovchick [5] studied a group of nearly 3500 patients and found no difference in survival rates whether response times were greater than or less than eight minutes.
Encouraging lower response times may lead to EMS workers choosing to use lights and sirens in situations where the patient is stable. Lacher and Bausher [6] found that EMS workers serving a pediatric hospital used lights and sirens inappropriately in almost 40 percent of the calls in which lights and sirens were used. While the reasons for this were not identified, it was found that EMS workers with lower levels of training were more likely to engage lights and sirens inappropriately than were more highly trained and certified paramedic personnel. Lacher and Bausher theorized this may be because the more novice EMS workers were less comfortable with providing care en-route and wanted to discharge the patient to a facility that could provide more effective care as quickly as possible. While the effect of inappropriate lights and sirens on crash rates is largely unknown, a study by Sanddal, Sanddal, Ward and Stanley [7] found a relationship between increased crash rates and the use of warning devices.
1.3. Ambulance Crashes and Transportation Mode
Sanddal et al. studied ambulance crashes that occurred between May 2007 and April 2009, identifying 409 separate crashes from the EMS Network database. Of the ambulance crashes for which information was available about the use of warning devices (lights and/or sirens) at the time of the crash, 77 percent occurred while lights and/or sirens were in use. All of those crashes resulted in injury or death [7].
The majority of crashes resulting in injury occur while the ambulance is in an emergency state and with the injured parties unrestrained prior to the critical event [8,9]. When an ambulance is involved in a collision, individuals in the rear of the vehicle (generally EMS workers and patients) show higher fatality and injury rates than those driving or riding in the front [8]. The higher injury and fatality rate in the rear cabin is related to the greater number of people in the rear of the cabin as well as reduced rates of restraint use in the rear patient compartment.
The ambient traffic, or the vehicles that are traveling in proximity to the EMV, is also at risk for crashes. A “wake effect” has been described in which an EMV using lights and sirens causes other vehicles to collide without actual physical involvement of the EMV. These crashes are difficult to track, but Clawson et al. [2] found potential wake-effect crashes that numbered more than five times the number of crashes that physically involved an EMV.
The patient care data collected in this study allowed researchers to perform analysis in an emergency transportation environment in order to assess transportation modes used by EMS workers providing patient care in patient transports. The objective of this study was to highlight and explore any contributing effects that specific patient illnesses have on ambulance operation in emergency mode. Understanding the relationship between transportation mode and patient condition could help to influence standard accepted response times and to aid in training EMS workers or dispatch personnel about appropriate conditions for using lights and sirens during patient transports, potentially reducing EMS crash rates.
2. Method
2.1. EMS Agency
The agency that provided records detailing patient care was the American Medical Response (AMR) ambulance service in Bozeman, Montana. Bozeman AMR is a paid, advanced life support (ALS) emergency care provider, serving a population of almost 100,000 people and responding to an average of 219 calls per month.
2.2. Patient Care Records
Data used in this analysis was collected from Patient Care Records (PCRs) provided by Bozeman AMR. A PCR is filled out as part of standard protocol for every patient transport, and its contents detail specific information pertaining to patient illness and medic responsive activities while under the care of an EMS worker. Institutional Review Board approval was granted for this study, and all data provided by AMR Bozeman was censored to eliminate any identifying patient or location information. The record set used for analysis includes all PCRs submitted by AMR between July 2, 2005, and July 1, 2010. This data set represents 13,253 individual calls. Table 1 shows a selection of relevant fields from those records along with a description and examples of data entry values from the PCRs.
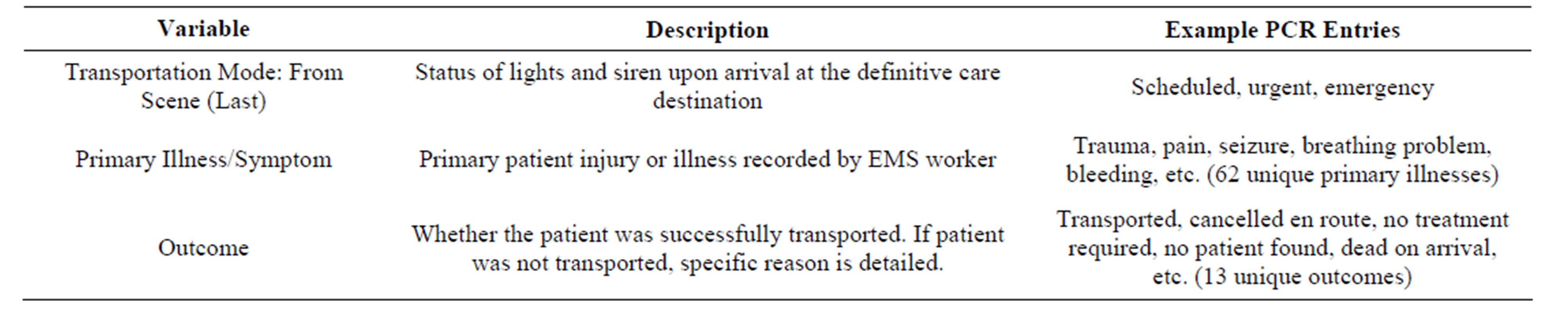
Table 1. Patient care record variable descriptions.
Transportation Mode is a categorical variable, indicating the emergency status of the ambulance during travel. Primary patient illness is the primary injury that resulted in the need for EMS care or transportation. Each patient transport is associated with only one primary illness.
2.3. Data Reduction
Of the 13,253 PCRs examined, the only records included in this analysis were those with an outcome of “Transported,” which excluded 3802 records. Excluded patient outcomes include “Patient Refused AMA” (2345 records excluded), “Cancelled FD/PD” (702), “Cancelled ENR” (386), “Dead On Arrival” (97), “No Patient Found” (84), “No Treatment Req’d” (53), “Lift Assist” (48), “InterFacility” (29), “Treated and Pronounced” (26), “Police Custody” (17), “Treat/No Trans”. (14), and “Helicopter” (1). Other records excluded were those in which the primary illness section of the form was not filled out (76 records excluded).
Data were adjusted to more specifically define transportation mode. As shown in Table 1, there are three outcomes for transportation mode: scheduled, urgent, and emergency. This analysis treated transportation mode as a binary variable (emergency/non-emergency), combining scheduled and urgent calls as “non-emergency” trips where lights and siren were not used.
2.4. Data Analysis
Initially an inflated binary logistic regression model was built including all levels of patient illness as predictor variables. A definitive model could not be built due to quasi-complete separation of data. This was evident in the data for the patient illness “Nausea”. There were 229 instances where nausea was the primary patient illness, but there were zero instances where nausea was the primary patient illness while the ambulance traveled in emergency transportation mode.
The Proc Logistic procedure was applied in SAS (version 9.3) to build a binary logistic regression model using the remaining variables to predict the binary response (emergency transportation mode vs. non-emergency transportation mode).
 (1)
(1)
where:
π represents the probability of experiencing emergency transportation mode;
 is referred to as the odds ratio;
is referred to as the odds ratio;
 is a parametric change in the odds ratio associated with a the presence or absence of the predictor i, such that
is a parametric change in the odds ratio associated with a the presence or absence of the predictor i, such that  is the change in odds of an occurrence associated with the presence of that predictor [10];
is the change in odds of an occurrence associated with the presence of that predictor [10];
xi is the presence or absence of the predictor i.
Significant predictors are reported along with their odds ratios and confidence intervals on those odds ratios. Patient illnesses that were not evaluated in the regression model due to separation of data and under-represented events were analyzed separately to determine if each response was overrepresented in emergency or non-emergency transports. Because the contingency table cells have both very small (event) and very large (non-event) values, neither Chi-Square nor Fishers’ Exact Test was possible, but the percent association is reported.
3. Results
Primary Patient Illnesses Contributing to Emergency Mode
All patient illnesses that had zero events in either emergency or non-emergency mode were dropped from the model. Dropped illnesses include shock (1 observation), “Behav/Psych” (229), “Nausea” (126), “Vertigo” (54), “Fever/Flu” (44), “CP-Musc/Skeletal” (35), “Epistaxis” (20), “Hypertension” (20), “Dehydration” (18), “Diarrhea” (18), “Swelling” (16), “Hypothermia” (14), “Eye Problem” (12), “Malaise” (8), “Environmental Injury”(4), “Mass/Lesion” (3), “Newborn”(3), “Contagious Disease” (1), “Device/Equip Prob”. (1), “Drainage/Discharge” (1), and “Not App”. (10). Shock was only observed during emergency transportation mode, and the remaining dropped patient illnesses were observed only during nonemergency transportation mode.
The patient illnesses that were found to be significantly higher odds of being transported using lights and siren included airway obstruction (odds ratio: 5.7 times more likely to use lights and siren), altered level of consciousness (2.3), breathing problems (2.3), cardiac arrest (262.3), cardiac symptoms (4.0), chest pain (2.9), congestive heart failure/pulmonary embolism (9.2), heart/cardiac illness (9.8), condition not entered on paperwork (3.1), obstetric conditions (7.4), respiratory arrest (66.4), respiratory distress (5.4), stroke/cerebrovascular accident (3.8), trauma (2.8), and unconscious patient or unknown condition (16.0). Figure 1 should be interpreted as follows: a transport with a patient whose primary illness is “Airway Obstruction” increases the likelihood of emergency transportation over non-emergency transportation mode by 100.75, or 5.7 times.
4. Discussion
Identifying patient illnesses that increase the likelihood of emergency mode transport can be helpful to EMS workers who may not have the experience or ability to quickly assess patient condition or whether that condition requires the use of lights and siren during transport. Illnesses that were found to be associated with higher likelihood of transportation using lights and sirens include: airway obstruction, altered level of consciousness (LOC), breathing problems, cardiac illnesses, respiratory illnesses, stroke, trauma, chest pain, obstetric illness (OB), and congestive heart failure or pulmonary embolism (CHF/ PE). This information is largely known or suspected by the EMS community, but this analysis objectively substantiates that knowledge.
While lights and siren can be used to reduce the time transporting a patient to definitive care, the interval of time between the initial call for assistance and the ambulance arriving on-scene is also important. The list of critical illnesses generated in this study can also be of use to dispatch personnel who inform responding EMS workers about the status of the patient prior to their arrival on the scene. For example, if a patient requested assistance with a primary complaint of nausea (0 of 226 patient transports due to nausea used lights and siren), the dispatch personnel could pass the information on to the responding EMV so they could travel to the patient without using lights and siren. An EMS dispatch coding system is already in use; however, there is some discrepancy in how dispatch personnel classify patient condition and severity compared to on-scene responding EMS workers. Neely et al. [11] studied whether EMS dispatch codes were equivalent between dispatch and the responding paramedic and found a trend of dispatcher “overcoding”, where the dispatch-assigned code was more severe than the code assigned by the paramedic. It was unclear whether this overcoding was due to excessive dispatcher caution or existing protocol. The trend that Neely observed may have also been evident in our transportation data— while only 5.4 percent of patient transports from the scene to definitive care used lights and siren, almost 87.4 percent of the travel en route to the patient was conducted in emergency mode. However, we cannot attribute this discrepancy to dispatch code assignment; our data set does not include the specific dispatch codes, only the mode of transportation that could have been chosen by EMS workers independently of dispatch information. An objectively generated list of illnesses requiring urgent response may be of use to help dispatch perform more accurate assessments about the urgency required in requests
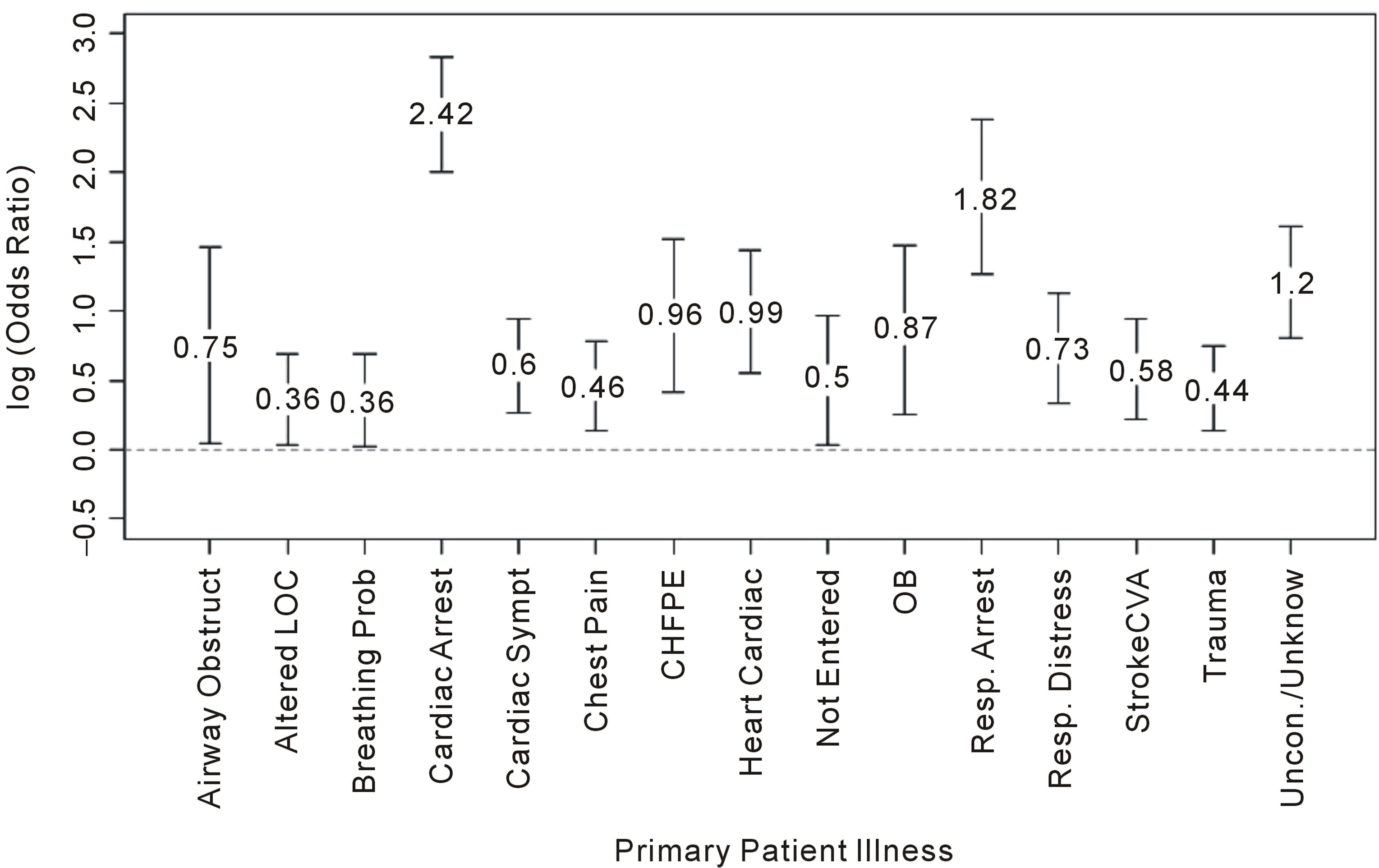
Figure 1. Log odds ratios and 95% CIs for association of patient illnesses with lights and siren.
for EMS response, thus minimizing the number of EMS responses using lights and siren. Additionally, patient illnesses that may not require immediate medical attention can be referred to medical advice hotlines or alternative EMS services in order to keep EMS resources available to respond to more critical patients.
A study by Maio et al. [12] that examined data from EMS transports collected survey responses from experts detailing several aspects of patient outcome, including a “survival” metric for different illnesses. An interesting extension to Maio’s study could be an examination of high “survival” scores (indicating illnesses where the impact and relevance of survival is important) and their relationship with frequency of transport using lights and siren. Results from such an analysis could identify illnesses that do not have an impact on patient survivability but that commonly lead to transports using lights and siren.
The purpose of using lights and siren during response and patient transportis to reduce emergency call response times. However, the time saved by using lights and siren may not be clinically significant. Studies that have compared EMV response times for emergency and non-emergency transport have found time savings as small as 43.5 seconds [13]. A more recent study found a larger time savings of 2.62 minutes [14]; however, this was not found to improve patient outcomes where patient care was administered in the ambulance. The current eight-minute goal for response time exists because of a study that focused specifically on cardiac arrest patients and their outcomes in relation to transportation time [3]. The list of patient illnesses enumerated in our study contains more than cardiac arrest and related symptoms. Further research should be performed to see if EMS response to these additional illnesses is being conducted with the appropriate warning measures (lights and siren when patient is not stable), or if the standard for response time should be adjusted to account for the time-critical responses needed for the additional patient illnesses.
One studied phenomenon associated with emergency mode is the existence of wake effects, which describe the higher rate of crashes among nearby vehicles that appears to be caused by the emergency vehicle operating with lights and sirens [2]. While the causes of this wake effect have not been explicitly identified, it is hypothesized that the crashes are due to the emergency vehicle’s lights and sirens affecting the actions of drivers in surrounding vehicles. With proper training, knowing which patient illnesses require lights and sirens could help EMV operators minimize the time spent operating in emergency mode inappropriately, potentially limiting wake effect crashes. Analysis of trends describing which patient illnesses are generally associated with emergency mode could help to identify potential “offending” illnesses—that is, illnesses that are thought to require emergency response but for which emergency response does not actually affect the patient survivability rate. Training could be especially beneficial for novice EMS workers, who may tend to inappropriately engage lights and siren [6] because they are not comfortable deciding which illnesses explicitly warrant the use of lights and sirens during transport.
4.1. Future Studies
Another application of these findings would be for researchers to compare the interactions of the EMS agency studied here with EMS groups in different population and geographical areas. Collecting the data used in this analysis required minimal effort, as it is already kept in electronic formats for billing and legal purposes by the EMS agencies.
4.2. Limitations
The data analyzed in this study were from a single EMS care provider, and so inference cannot be made to a broader patient group than that found in Bozeman, Montana, as the distribution of patient illnesses and injuries seen in this study may be specific to AMR Bozeman’s service area. However, the data used in this study are typically maintained by most major healthcare providers for billing purposes, so other agencies should be able to reproduce the analysis quickly. Information on dispatch codes was unavailable for study. Without this information, analysis was not able to be conducted regarding the agreement of emergency or non-emergency coding between the EMS workers and dispatch. The data were gathered from paperwork filled out by EMS workers during and after patient transportation, so it is possible that there are some paperwork errors or omitted data points. Finally, because information describing specific EMS worker training level was not available, assessment of the effect of EMS training level on whether or not transports used lights and siren was not possible.
5. Conclusion
This study presents a list of illnesses that frequently result in patient transports using lights and siren. While previous studies focus mainly on cardiac injuries, these findings suggest that survivability studies related to transport time and mode of transportation should be expanded to include respiratory illnesses. The list of illnesses highlighted here will additionally be helpful in training novice EMS workers or dispatch personnel who may lack the expertise or confidence to appropriately and quickly assess patient condition, resulting in less frequent travel with lights and siren, thereby increasing transportation safety.
Abbreviations
EMS: Emergency Medical Service EMV: Emergency Medical Vehicle ALS: Advanced Life Support PCR: Patient Care Record LOC: Level of Consciousness OB: Obstetric CHF/PE: Congestive Heart Failure or Pulmonary Embolism