Prevalence and Factors Associated with Preoperative Anxiety during COVID-19 Pandemic at Tertiary Care Center ()
1. Introduction
Anxiety is defined by the American Psychiatric Association as a subjective experience of unease, discomfort, apprehension, or apprehensive concern accompanied by autonomic and somatic signs (Abuse, 2016) . Exaggerated alertness can be brought on by anxiety, which frequently comes with physical and psychological symptoms like agitation, exhaustion, muscle tightness, perspiration, tachycardia, elevated blood pressure and intrusive thoughts (Sigdel, 2015) (Stamenkovic et al., 2018) . The symptoms of anxiety disorders are varied and include everything from hyperarousal to trouble concentrating (Neuroscience et al., 2013) . This can lead to subjects opting out or postponing the surgery that can eventually affect the health outcome of the patient. In addition, the surgeon can cancel the surgery when the patient is hemodynamically unstable.
Most people experience transient anxiety before and after surgery since it is a stressful event.
Preoperative anxiety is a common reaction that is linked to both mental and physical health issues (Jawaid et al., 2007) . Preoperative anxiety that is at an excessive level can have major consequences, including an increased chance of postoperative problems like discomfort, a protracted recovery period, extended hospitalization, and death (Kain et al., 2006) .
Anxiety disorders are thought to affect 4.05% of people worldwide (Javaid et al., 2023) . Preoperative anxiety was predicted to be present in 55.7% of surgical patients in LMICs (low/middle-income countries) (Bedaso et al., 2022) . The COVID-19 virus is linked to an increase in fear and anxiety in people everywhere (Gupta et al., 2020b) . According to research done in Nepal during the pandemic, 38% of the healthcare professionals assigned to COVID-19 duty had anxiety and/or depression (Gupta et al., 2020a) . Preoperative anxiety is present in 11% of patients due to COVID-related variables (Viola et al., 2021) . The purpose of this study was to assess how the pandemic affected the emotional well-being and fear of SARS-CoV-2 transmission in a cross-sectional study of Nepalese patients scheduled for surgery during the COVID-19 pandemic.
2. Methods
2.1. Study Design and Setting
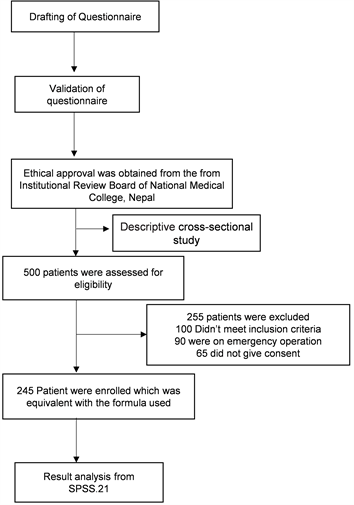
This was a cross-sectional descriptive study which was conducted at National Medical college, a tertiary care center. All in-patients who were planned to undergo all major operative procedures from May 2021 to April 2022 were enrolled. All the patients signed a written consent before participation. The Sample size was 245.
2.2. Sample Size Calculation
Sample size was calculated using the formula:
n = required sample size 0.659
t = confidence level at 95 %
P = prevalence of anxiety in preoperative patient (20 % i.e. 0.20) (Kain et al., 2006)
m = margin of error at 5%
Sample size – Sample size will be 245.
2.3. Eligibility Criteria
Inclusion criteria:
1) All surgical patients between ≥ 18 to 60 years of age.
2) Patient undergoing elective surgery in spinal or general anesthesia.
3) All in-patient admitted in ward.
4) Patients willing to give consent.
Exclusion criteria:
1) Patient below 18-year-old and more than 60 years of age.
2) Patients undergoing emergency surgery.
3) Patient diagnosed with any form of mental illness prior to current admission
4) Patient under psychotropic and anxiolytic drugs.
5) Patient with any form of cognitive decline like dementia or delirium or any causes of brain damage.
6) Patient who does not have insight about surgical procedure and incapable to understand and respond to the questionnaires.
2.4. Data Collection and Instruments
The data were collected using validated and standardized anxiety measuring tools like Beck Anxiety Inventory (BAI) and General health questionnaire-12.
Beck Anxiety Inventory (BAI) (Adhikari, 2019) : It consists of 21 questions. It has been commonly used to assess anxiety in populations. It is a self-report tool for anxiety. Each question is scored from 0 to 3. For interpretation of total scores, 0 - 21 is considered low or normal anxiety, 22 - 35 is moderate anxiety and for severe anxiety score must be more than 36. The tool was translated into Nepali and back-translated into English and several iterations were done till the original meaning was obtained.
General Health Questionnaire-12 (GHQ-12) (Goldberg et al., 1997; Donath, 2001; Joshi et al., 2021) : The GHQ-12 consists of 12 items, each of which is evaluated by four indexes. The tool was translated into Nepali and back- translated into English and several iterations were done till the original meaning was obtained. Total scores range from 0 to 36 with a score of 11 or 12 considered typical, scores > 15 suggesting evidence of distress, and scores > 20 are considered severe problems with psychological distress.
2.5. Data Processing and Analysis
Data was entered manually into Microsoft Excel and Statistical Package for Social Science (SPSS.21). Any value of p < 0.05 was considered significant.
2.6. Ethical Considerations
Ethical approval was obtained from Institutional Review Board of National Medical College, Nepal. Researchers used to be informed in every department where surgery has been recommended. Next, patients were contacted about the research via staff. If a verbal consent was given, the patient will be informed both verbally and in written about the research. Participants had some time to consider taking part before the researcher returned to discuss more about the study. If individuals consented to participate in the study, they had to give their written consent. After obtaining written informed consent, we enrolled 245 patients undergoing elective surgery between May 2021 to April 2022 at National Medical College Teaching Hospital, Birgunj, Nepal.
Flow Chart Showing the Enrollment:
3. Results
Information on the descriptive characteristics of the patients is given in Tables 1-3. Total of 245 surgical patients participated in the study. One hundred thirty
![]()
Table 1. Respondents’ Socio-demographic variables (n = 245).
![]()
Table 2. Factors affecting preoperative anxiety.
Significant: p < 0.005.
![]()
Table 3. Respondents’ level of pre-operative anxiety (n = 245) (BAI) (GHQ12).
(53.1%) of the participants were male and majority (67.3%) belong to the age of 18 - 39 years. 62.4%, 33.9%, and 44.9% 26.5% were in fear of preoperative pain, anesthetic agent, anesthetic pain and fear of not awaking respectively. About 74.3% of patients received preoperative pain information; nonetheless, 75.5% of patients reported being satisfied with their knowledge. According to the BAI, 90.2% and 9.8% of respondents reported mild and moderate anxiety respectively, and the GHQ 12 found that 88.6% of respondents had typical problems, 6.9% had distress and 4.5% had severe problems with psychological distress. According to the BAI total score averages (p > 0.05), there was no statistically significant difference between types of anesthesia, surgical complication in family, worried about infected with COVID, stressor in family, fear of anesthetic pain and fear of not awaking. However, there was a statistically significant difference (p < 0.05) between BAI total score and types of surgery, history of previous surgery, history of substance abuse, history of medical illness, fear of preoperative pain, fear of postoperative pain, fear of anesthetic agent, fear of not awaking, preoperative information given about pain and patient satisfaction with preoperative counseling.
4. Discussion
Anxiety is usually felt before surgery and is generally considered normal. Although preoperative anxiety and its cause have been studied, research on how it affects during COVID-19 in Nepal is still lacking. Anxiety before surgery could be identified and managed. In our study, 30.2 % of the study population had anxiety. No one experienced severe level of anxiety which is similar to the study conducted by Ganga Prajapati in TUTH, Nepal (Prajapati et al., 2022) . In the study conducted in Italy during COVID-19 pandemic among neurosurgical patients scheduled for non-urgent surgery, 18.9% of the participants displayed signs of anxiety (Doglietto et al., 2020) which is more in study conducted in India i.e., 25% (Viola et al., 2021) . This study’s prevalence is higher because it was carried out in Nepal during the lockdown and immediately after the lockdown. Additionally, this discrepancy could be caused by the sample size, time lag, and anxiety-accessing metrics. In this study, we identified factors affecting patients' anxiety scores. The causes of pre operative anxiety among the respondents were found to be related with fear of preoperative pain 62.4%, which is contrast to the study done in Teaching Hospital of Ethiopia (Ferede et al., 2022) which was only 39.9%.
In our study, fear of not waking up is 26.5% and 36% in study conducted in Rupandehi, Nepal (Dhungana et al., 2019) but was more in study of Ethiopia which was 58.4% (Nigussie et al., 2014) . Fear of anesthetic pain is 44.9%, inadequate preoperative information 21.6% and patient partially satisfied with counselling about operation 18.8%. In this study fear of post operative pain, fear of anesthesia was 59.2%, 33.9% which in study done in Ethiopia was 60.9%, 65.7% (Bedaso & Ayalew, 2019) . Fear of pain after surgery was slightly less in Jordan and Turkey which was around 34.5% (Aloweidi et al., 2022; Celik & Edipoglu, 2018) . This discrepancy in findings may be explained by the possibility that patients in our study did not receive adequate counseling regarding postoperative pain management techniques, in contrast to other facilities where counseling services were more effective in lowering patients’ fears of postoperative pain.
Preoperative psychological counseling as well as preoperative medicine is advantageous for people with higher preoperative anxiety since all the contributing factors have heightened anxiety levels, which can be decreased (Akkamahadevi & Subramanian, 2016) . For example; frequent and effective communication, providing information about the surgical procedure in general, about the type of anesthesia used, possible complication of the procedure, the benefit of surgery, active listening, personal visits, medication, etc. Exercises for relaxing the muscles or deep breathing can also be taught.
According to our study, 33.5% people were worried about being infected with COVID-19 during hospitalization which was more compared to Jordanian population i.e. 21% (Aloweidi et al., 2022) . This discrepancy resulted from the public’s noticeably rising worry over COVID-19 and coronavirus restrictions at the time. Unexpectedly, there was no significant association between preoperative anxiety and worried about getting infected with COVID-19. This is similar to the study done in India (Viola et al., 2021) . Our study highlighted the most significant factors contributing to preoperative anxiety by preoperative pain, postoperative pain, fear of death which was similar to study done in Jordanian and Turkish people (Aloweidi et al., 2022; Celik & Edipoglu, 2018) .
5. Conclusion
In conclusion, this study demonstrated that 30.2% of patients had preoperative anxiety. Fear of preoperative pain, fear of postoperative pain, fear of not awaking was related to preoperative anxiety. This suggests that preoperative counseling about these factors can play a crucial role in decreasing preoperative anxiety. Although the current study suggests that there is no significant correlation between BAI score and COVID-19 infection, around one-third of the patient were afraid of contacting COVID-19 during hospital stay, for which controlling the spread of COVID-19 by implementing all preventive measures can also play a role in decreasing preoperative anxiety during this pandemic.
6. Limitations
The limitations of this investigation were several. We were unable to assess preoperative anxiety at other tertiary teaching hospitals because our study was a single-center study. Due to the need for a modified study design for this patient population, we did not include patients undergoing emergency procedures. This study excludes patient with chronic medical and psychiatric illness.