1. Introduction
Split hand/foot malformation (SHFM), formerly known as ectrodactyly is a rare congénital anomaly, its incidence varies from 1/8500 to 1/25.000 live birth [1]. Several cases have been reported throughout the world, with China reporting the highest prévalence [2]. In our country, no publication on this subject has been found. The malformation of split hand and foot mainly affects the development of the limbs, its clinical variability is standard, can present as an isolated feature or as a syndrome associating other congenital anomalies. The prognosis depends on the type of anomalies. We report two (2) cases with different clinical presentations and prognoses for which a genetic origin is probable.
2. Medical Observation
This is a newborn male admitted on the 3rd day of life for the management of a malformation syndrome. His father, 40 years old, carrier of anomalies of the 4 limbs with the type of split feet and hands, presents a moderate functional incapacity of the hands (Image 1 and Image 2). Her mother, 38 years old, has no visible external malformations. The couple is not consanguineous, is of the same ethnic group, there is no exposure to toxic chemicals and has 3 children in apparent good health, without malformations. The pregnancy was well monitored and brought to term. An ultrasound performed at 36 weeks of amenorrhae did not find any abnormality. At delivery several external malformations were noted (Image 3 and Image 4).
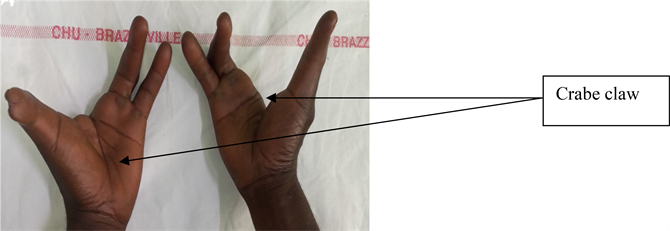
Image 1. Bilateral median split on the thoracic limbs.

Image 2. Bilateral median split on the pelvic limbs.

Image 3. Bilateral digital hypoplasia of thoracic limbs.

Image 4. Bilateral median split on the pelvic limbs.
The review also revealed,
· sucking: slow rhythm, rare swallowing movement;
· macrognathia, gingival hypoplasia, hypoplasia of the tongue;
· suspicion of a cleft palate under the mucous membrane;
· fine and sparse hair, the skin is dry.
Cardiovascular, respiratory and abdominal examination showed no anormalities. The paraclinical examination notably radiography of the limbs, abdominal ultrasound and blood samples for genetic analysis not performed due to our limited resources setting. We evoked the syndromic form in the newborn with difficulties in breast feeding complicated by weight loss.
The management consisted of the administration of breast milk through a nasogastric tube, a syringe or a cup. The baby was discharged from the hospital at 21 days of life and weighed 3000g. He is regularly reviewed in the department, currently 17 months old and weighs 10kg.The surgical management of the cleft palate is still pending.
3. Discussion
Split hand/foot malformation (SHFM), formerly known as ectrodactyly, is a heterogeneous group of congenital limb anomalies of genetic or environmental origin [1]. The mode of transmission is variable autosomal dominant mainly but have also been described, autosomal recessive mode, X-linked recessive inheritance and sporadic cases without family history resulting from de novo mutation, duplication and deletion, some rare cases have been attributed to teratogens, in particular exposure of the embryo to retinoic acid [3]. The main pathogenic mechanism is the failure to maintain medial apical ectodermal ridge (AER) signaling, resulting in defects of the central rays of the hands and or feet [4]. The incidence of SHFM ranges from 1/8500 to 1/25.000 live births [1].
Antenatal diagnosis is possible from the first trimester onwards thanks to ultrasound [5]. The diagnosis is guided by the existence of risk factors. In our case the mother was not a carrier of anomalies, and the father's anomalies were not known to the midwife, so ultrasound was not indicated. According to the clinical expression, SHFM presents as a median cleft of the hand or foot, hypoplasia/ aplasia of one or more phalanges, central metatarsals or metacarpals making the characteristic lobster claw appearance, associated with syndactyly which was the case of the patients presented. These anomalies may be limited to one limb [6] [7] in this case the thoracic limb is most often affected [2] [8] or involve all 4 limbs [9] [10], as was the case with the patients presented. SHFM are classified into isolated and syndromic forms [1] [2], The limb abnormalities present in the newborn are distinct from onelimb to another and also from those father, this interindividual and intrafamilial clinical variability is the rule in the SHFM. The abnormalities present in the father being only of the split hands and feet type, this was an isolated form. Syndromic forms combine limb and extra-limb disorders. The most frequently described syndromes are: EEC syndrome (ectrodactyly-ectodermal dysplasia-cleft lip/palate syndrome), EEC syndrome without cleft lip/palate, LADD syndrome (lacrimo-auriculo-dento-digital syndrome), ADULT syndrome (acro-dermato-ungual-lacrymal-tooth syndrome), CHARGE syndrome or VATER association [1]. The newborn with split hands and feet (SHFM) and extra-limb defects such as hypo-retroglossia, macrognathia, thin and sparse hair, cleft palate and dry skin presents a syndromic, similar to EEC syndrome with cleft lip. The syndromic triad of the EEC being split hand/foot; cleft lip or palatine and ectodermal dysplasia, here represented by skin and hair anomalies [1] [11]. Cytogenetic and/or molecular tests are necessary to provide confirmation. In our case, the abnormalities found in the father and son suggest a probable genetic origin [9] [12] [13].
In isolated SHFM with only finger anomalies, the problem is the functional incapacity of the hand caused by the severity of the damage; whereas in syndromic forms the severity is not only related to the functional incapacity of the hand but also to the associated anomalies [1]. In our case the newborn presents with microglossia and backward retraction which causes difficulties in sucking and has resulted in a weight loss of more than 10% in 3 days.
Reconstruction of the split hand is possible in forms with functional incapacity [13], associated anomalies are subject to specific management. In our case, traction of the tongue is necessary to restore its function of sucking and swallowing. This depends on the nutritional status and is planned when the child weighs at least 8 kg, in collaboration with the SOS Smile association.
4. Conclusion
SHFM in its isolated or syndromic forms presents a variability of clinical expression that affect prognosis. The familial forms are suggestive of a genetic origin. Molecular understanding is necessary in order to prevent recurrences.