Eating Habits among Lithiasic Patients in Kinshasa, the Democratic Republic of Congo ()
1. Introduction
Urolithiasis is a common health problem with a multifactorial etiology arising from the interaction of various factors including metabolic, genetic, and environmental [1]. Calcium oxalate accounts for the majority of kidney stones [2]. Over the last decades, urolithiasis incidence has been increasing worldwide at an alarming rate [3]. Several factors such as age, gender, race, nutrition, daily water intake, climate, geography, physical activity and Body Mass Index (BMI) play a key role in urolithiasis pathogenesis [4]. Early studies showed that nutrition contributes substantively to kidney stone formation [5] [6]. Prior evidence reported that high dietary calorie, animal protein and oxalate intake and low daily water intake, calcium and potassium consumption correlated with higher incidence of calcium oxalate stone formation, thus representing important risk factors in kidney stone formation [7] [8]. Therefore, dietary investigation represents an important step in the etiological investigation of urolithiasis [9]. Despite a wealth of studies investigating the association between kidney stone formation and nutrition habits, data on the nutritional status and dietary habits of patients afflicted with kidney stones in the Democratic Republic of Congo (DRC) are lacking. To fill this gap, the present study was designed to determine the dietary habits of patients who followed for urolithiasis in the city of Kinshasa and to evaluate the association between dietary habits and the composition of the stones.
2. Material and Methods
2.1. Study Design and Setting
This was a dietary survey conducted from January 2017 to September 2019 among lithiasic patients attending 8 hospitals in the city of Kinshasa. In this case study, the sample size was not predetermined in its initial phase and the study focused on lithiasic patients for the most part easily accessible in hospitals that agreed to collaborate in this study. Thus, 85 patients had taken part in the study. Only the patients followed in these hospitals for urolithiasis who agreed to freely answer the questionnaire for this survey had taken part in this study.
2.2. Dietary Survey
The final report of the study on the identification and evaluation of the nutritional quality of food supplements in use in the DRC carried out by the non-governmental organization GAAD with funding and technical support from UNICEF [10] was used as a reference for the validation of this survey. Different foods commonly consumed in the DRC were categorized according to their composition: foods rich in animal proteins (beef, pork, goat meat, smoked meat, offal, chicken thighs, turkey rump, chicken, and others), foods high in salt (salted fish, cold meats, cans and others), foods rich in calcium (cow’s milk, cheese, yogurt and others), foods high in sugar (sugary drinks, juices and other soda), foods rich in oxalate (peanuts, peanut feet, sorrel, spinach, eggs, chocolate and others) and various vegetables and fruits.
We then established a scale from 1 to 4 according to the frequency of consumption of these foods: occasional consumption of a food was rated 1, consumption once a week was rated 2, while consumption 2 to 3 times a week was rated 3, and a daily consumption was rated 4. Ratings 3 and 4 were categorized as heavy consumers of a given food.
We also evaluated daily water intake. This frequency was qualified as “a lot” when the patient took water several times during the day (quantity estimated at more than 1500 mL/d), “Not much” when the patient took water twice during the day (quantity estimated at 1000 to 1500 mL/day), finally “hardly” when there was only one dose during the day (quantity estimated at less than 1000 mL per day).
2.3. Infrared Analysis of Stones and Study Parameters
The different layers of stones were analyzed by Fourier transform infrared spectrophotometry (Vector 22 FT-IR spectrophotometer, Bruker Optics, Champs-sur-Marne, France) in absorbance mode by accumulation of 32 spectra between 4000 and 400 cm−1, with a resolution of 4 cm−1. Stones were classified according to their main component (chemical or crystalline body representing the large proportion in a stone).
Patient demographic and clinical data were obtained from medical records and during the medical appointment, including age, sex, place of residence, weight and height to calculate the body mass index (BMI), occupation, site of stones, existence of a urinary tract infection, comorbidities, and serum creatinine. Age was divided into 4 categories: <20 years, 20 - 39 years, 40 - 59 years, and ≥60 years. The profession was categorized in 3 groups: civil servant, liberal, and student/pupil and unemployed.
2.4. Statistical Analysis
Continuous variables were expressed as means and medians. Categorical variables were summarized into proportions. Differences in categorical variables between groups were assessed using Chi square test or the chi-square likelihood-ratio as appropriate. Differences in means were assessed by the student’s t test. p values less or equal to 0.05 were interpreted as statistically significant. Statistical analysis was performed using SPSS Statistics software version 22 (IBM, Armonk, USA). This study was approved by the ethics committee of the School of Public Health at the University of Kinshasa (approval number: ESP/CE/29/2020).
3. Results
A total of 85 lithiasis patients attending various hospitals in Kinshasa participated in this survey. Demographics are summarized in Table 1. The mean (SD) age of patients was 47.1 (14.0) years. Most participants were males (63.5%, n = 54). Sixty-four patients (75.3%) had stones located in the upper urinary tract. Females had more upper tract stones compared to males (90.3% vs. 66.7%, p = 0.012). The vast majority of patients (85%) were residents of Kinshasa.
While 6 (7.1%) patients were undernourished, 46 (54.1%) were overweight or obese. Just over a quarter of patients (25.9%) had a urinary tract infection and Escherichia coli was the most frequently isolated bacteria. Twenty patients (23.5%) had hypertension and 9 (10.6%) had impaired renal function (Table 2).
![]()
Table 1. Sociodemographic parameters by the site of stones.
*Pearson chi-square.
![]()
Table 2. Clinical parameters according to the site of the stones.
*Pearson chi-square.
Most patients (77.6%, n = 66) consumed vegetables and fruits. Other dietary habits found in these patients were excessive consumption of animal proteins (62.4%, n = 53), heavy consumption of sugary drinks (58.8%), consumption of foods rich in oxalate (58.8%), high consumption of foods rich in calcium (40%), and a salty foods (34.1%). Most patients (68.2%) drank less than 1500 mL of water in 24 hours.
Females consumed more salty foods than males (48.4% women vs. 25.9% men, p = 0.032). Apart from the high-salt diet, we did not note any statistically significant differences between the eating habits and sex of the patients. Young adults consumed more sugary drinks than other age groups (83% young adults vs. 59% adults and 23.5% people over 60, p = 0.002) (Table 3).
![]()
Table 3. Eating habits by sex and age.
*Pearson chi-square, the p correspond to the distribution of eating habits according to sex and age groups of patients.
Patients residing in the provinces of the DRC had a saltier diet (64.3% outside Kinshasa vs. 28.2 Kinshasa, p = 0.012) than those residing in the city of Kinshasa. People from the western and northern provinces consumed more sugary drinks than those from other DRC provinces (66.7% West and 80% North vs. 41.4% Center-South and 40% East, p = 0.041) (Table 4).
Only the stones of 61 out of the 85 patients who took part in this dietary survey were extracted during our study period and analyzed at the TENON hospital (APHP, Paris, France).
The whewellite majority in the stones of 45 patients (or 73.8%) was the largest majority body. The other major bodies identified were carbapatite (in 6.5% of cases), weddellite (6.5%), struvite (4.9%), ammonium urate (4.9%) and l anhydrous uric acid (4.9%).
![]()
Table 4. Eating habits according to place of residence and province of origin.
*Likelihood chi-square, p correspond to the distribution of eating habits according to the residence and province of origin of the patients.
Anhydrous uric acid stones were completely associated with a high BMI (overweight) and 50% of carbapatite stones were associated with under nutrition (p = 0.025). No statistically significant difference was noted between the distribution of urinary tract infection and majority stone bodies.
Males with a diet rich in oxalate had more calcium oxalate stones (64.3%) compared to other major bodies (carbapatite, struvite and ammonium urate urate) (p = 0.041) (Table 5).
4. Discussion
Eating Habits and Chemical Composition of Stones
In this study, vegetable consumption was the most predominant diet. The other dietary habits found in these lithiasis patients included high consumptions of
![]()
Table 5. Majority bodies based on BMI, urinary tract infection and oxalate consumption in men.
*Pearson chi-square. CA: carbapatite, PAM: struvite, AU0: anhydrous uric acid and UrAm: ammonium urate.
animal proteins, consumptions of foods rich in oxalate, refined sugars, calcium, and consumptions of foods high in salt. Also, men with a diet high in oxalate had more calcium oxalate stones compared to other main stones.
Most of patients in this study (77.6%) had a diet rich in vegetables and fruits. Several studies have demonstrated the protective role of a diet rich in vegetables and fruits [11] [12]. Likewise, a Dietary Approaches to Stop Hypertension (DASH) diet, rich in fruits, vegetables, whole grains, and low-fat dairy products, has been shown to significantly reduce the risk of kidney stone formation [13]. However, it is worth mentioning that the protective effect of a diet rich in vegetables and fruits is only observed in people who rarely consume them [12]. Indeed, Meschi et al. [12] found that urinary citrate excretion was significantly reduced and calcium excretion was significantly increased after a two-week diet of vegetables in a normal population [12]. Furthermore, Daudon et al. [14] revealed that a vegetable diet is often rich in oxalic acid and poor in calcium, which would promote hyperoxaluria and the formation of calcium oxalate stones observed in developing countries. In this study, whewellite (73.8%) was the most frequent component and less than half of patients (40%) consumed foods rich in calcium. Thus, the need to examine the oxalate content in various green leaves and vegetables regularly consumed in the DRC.
In this study, 58.8% of patients had a diet rich in oxalate and a statistically significant association was found between a diet rich in oxalate and calcium oxalate stones in men. Higher consumptions of oxalate increase the risk of stone formation [15]. Oxalate, a terminal acid in metabolism whose primary route of excretion is the kidney, binds to calcium to form calcium oxalate which is an important lithogenic complex [9] [16]. Three potential sources of oxalate intake are known: foods rich in oxalate (represents 10% to 20% urinary oxalate) [9] [16], hyperoxaluria may be secondary to intestinal malabsorption [16] [17] [18] [19] and hepatic oxalate synthesis which depends on lean body mass (represents 80% to 90% of oxalate). However, a diet very low in oxalate can reduce urinary oxalate excretion by half [9] and only 100 - 1000 mg of free oxalate which is absorbed per day [9] [14].
Besides higher consumptions of vegetables, we also found that 62.4% of patients had a diet rich in animal proteins and 58.8% consumed refined sugars contained in juices and other soft drinks. Ferraro et al. [20] found that higher consumption of sugary drinks was one of the modifiable risk factors associated with urinary stones. There is also evidence that sugary and carbonated drinks increase the risk of urinary stone formation [21]. Zhuo et al. [11] reported that animal protein intake was significantly associated with the occurrence of urolithiasis. Short-term restriction of animal protein significantly reduces the excretion of calcium, phosphate, hydroxyproline, uric acid and oxalate and increases the excretion of citrate in the urine, reducing the risk of stone formation [22]. Therefore, patients with recurrent calcium oxalate urate stones should decrease consumptions of animal proteins and avoid foods high in purines.
It is known that calciuria is an important determinant of calcium lithogenicity because hypercalciuria is found in 30% to 60% of lithiasis patients. Calciuria is influenced by nutritional factors such as excessive salt, calcium, and proteins intake [9] [14] [16] [23] [24]. In this study higher intake of salt, calcium and proteins were found in 34.1%, 40%, and 62.4% of cases, respectively.
Milk, dairy products, and drinking water are the main sources of dietary calcium [9] [16]. Digestive absorption of calcium represents 20% of the amount ingested, or 5 mmoL/d (200 mg), and the kidney is the only way out of calcium. Any excess sodium intake in food leads to increased urinary calcium excretion. It is also known that the consumption of animal proteins is associated with the increased incidence of calcium urolithiasis. The multifactorial effects of excess animal proteins include: lowering of urinary pH, increased excretion of calcium, uric acid, oxalate and a decrease in citrate excretion. [14] [25] [26] [27] [28]. Thus, sodium intake must be maintained around 6 and 7 g/d; whereas protein intakes should be normalized to 1 g/kg/day in adults [29] [30].
This dietary survey revealed that 68.2% of patients drank less than 1500 mL of water per 24 hours. High fluid intake has been shown to increase urine volume, reduce the concentration of calcium oxalate in urine, and reduce the risk of stone formation by 50% and the recurrence rate from 60% to 80% [31] [32]. Indeed, Zhuo et al. [11] demonstrated that fluid intake was significantly associated with the occurrence of urolithiasis. We believe that lower water intake in our study is due, at least partially, by limited access to clean drinking water. Water intake should be harmoniously distributed throughout the day and adjusted according to the fluid losses. This could help prevent urolithiasis and reduce the frequency of recurrence [16] [31]. Remember that there are three categories of water; prepackaged natural mineral waters, prepackaged spring waters and water for public distribution (tap water), rainwater and well water; the latter being generally very low in calcium. Mineral and spring waters are the only ones that can take advantage of properties favorable to health, benefiting from an original nature and purity, coming from underground water free from any pollution, stable in their composition [9].
Finally, the small sample size of this hospital series is a limiting factor that must be taken into account in interpreting these results. But, beyond this possible limit, this study made it possible for the first time to describe the eating habits of lithic patients in the DRC.
5. Conclusion
In this study, high consumptions of vegetables and low water intake were linked to the formation of calcium oxalate monohydrate stones. More data are needed to confirm these findings.
Acknowledgements
The authors sincerely thank the Department of Functional Explorations of the Tenon Hospital in Paris, the staff of the Urology Department of the University Clinics of Kinshasa, as well as all the partner hospitals and doctors who agreed to collaborate with us in the context of this study.
Authors’ Contributions
PD, DM designed, collected, interpreted, wrote and corrected the manuscript. EM, AN analyzed the data, read and corrected the article. JRM, ML and ES read and edited the article, MD and PD carried out the morpho-constitutional analysis of stones, and revised the manuscript, APM, SL, MD and JPH supervised, interpreted and edited the article. All authors have read and approved the final version of the article.
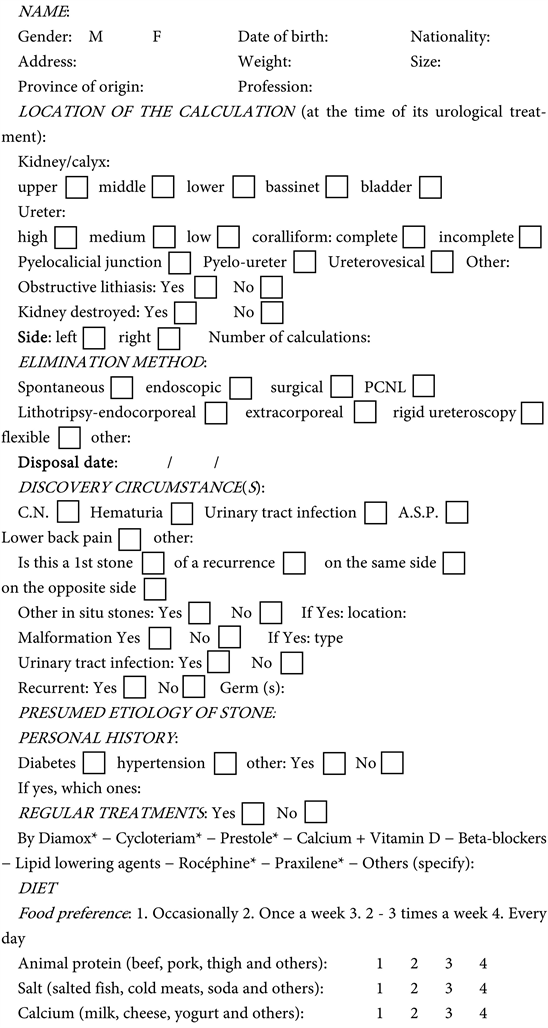
DATA COLLECTION SHEET: DIETARY SURVEY OF LITHIASIC PATIENTS IN KINSHASA.