Assessment of public awareness about body measurements among Fayoum population ()
WHO data were estimated for adults aged 15 years and the older from 16 countries in the Region and showed the highest levels of overweight and obesity in Egypt, Bahrain, Jordan, Kuwait, Saudi Arabia and United Arab Emirates. The prevalence of overweight and obesity in these countries ranges from 74% to 86% in women and 69% to 77% in men [4]. Egypt is the 14th fattest country in the world, according to (WHO, 2010) [5].
Overweight and obesity are defined as abnormal or excessive fat accumulation that presents a risk to health. Overweight and obesity are the fifth leading risk for global deaths. At least 2.8 million adults die each year as a result of being overweight or obese. Obesity is among the leading modifiable behavior risks for morbidity, mortality and disability [6].
Body Mass Index (BMI) has probably become the most common indicator used to assess overweight and obesity in a wide variety of settings, including clinical, public health, and community-based programs [7]. There was general agreement that BMI surveillance was a sound epidemiologic tool for the assessment of overweight and obesity in populations. It can be used to increase community awareness of need and to focus their attention on the importance of weight management [8]. The International Obesity Task Force (IOTF) cut points linked BMIs of 25 kg/m2 (adult overweight) and 30 kg/m2 (adult obesity) at age 18.0 years and above [9,10].
Community-based programs and educational strategies are designed to reach people outside of traditional health care settings. Using non-traditional settings can help to encourage informal information sharing within communities through peer social interaction. Reaching out to people in different settings also allows for greater tailoring of health information and education [11].
For a community to improve its health, its members must often change aspects of the physical, social, organizational, and even political environments in order to eliminate or reduce factors that contribute to health problems or to introduce new elements that promote better health [12].
Our primary goals were to explore level of community awareness about body measurement, assess prevalence of obesity among the Fayoum population, and examine actual body weight with self-perception of body image.
2. SUBJECTS AND METHODS
This study was a community-based research related to body measurement awareness because it is very important to detect the perception of individual to his body image, as this is the first step for problem solution is to be aware that there was a problem related to health status of the individuals. The study was a cross-sectional descriptive observational survey conducted in Fayoum Governorate, a developing city in Middle Egypt. We used multistage stratified random sampling to select the study household. In the first stage, the governorate was divided into 6 districts: (Fayoum, Etsa, Tamiya, Sinnuris, Youssef Sadiek, Abshoay). We choose Fayoum district because it has both an urban and rural population as it is surrounded by villages. Fayoum district population is estimated of 566; 164 inhabitants, according to (CAPMAS, 1996) [13]. Thus, they represent 5.28% of the total population of the province. In the second stage, two regions were selected Mansiat Abdallah and Mansiat Lotfallah based on the adjacent geographic location and they represent a rural and urban community. In the third stage two main streets were selected. In the fourth stage, the households were chosen by random sample in the chosen streets.
A study was carried among the population who were aged ≥16 years in the chosen households. A simple questionnaire was conducted on a random sample of 582 participants. A pre-designed structured questionnaire was used to collect the information regarding the socio-demographic profile of the population and their awareness about their weight, height and body mass index and waist circumference as a tool for detection of obesity. Anthropometric assessment was carried out according to Jelliffe (1966) [14]; weight, height and waist circumference were measured and BMI was calculated according to the following formula (Quetelet, 1830 to 1850): BMI = weight (kg)/height (m) 2. Weight: the participant was weighed wearing light cloths and without shoes, using digital balance. Height: was measured with the subject’s head in the Frankfort plane and without shoes to the nearest 0.1 cm; waist circumference: just above the pelvic bony (prominences) landmarks.
The following cut off values of BMI of 30 or more is generally considered obese and BMI equal to or more than 25 is considered overweight. As regards the waist circumference which is used to assess the abdominal obesity the cut off values for women: WC > 88 cms and WC > 102 cms for men [15].
2.1. Statistical Analysis
Data Management: Data were collected, coded and analyzed using Statistical Package for Social Science (SPSS) software version 18 (SSPS, Chicago, IL). The prevalence was expressed in percentage. In addition to descriptive statistics, non-parametric tests (chi-square) were used to find its association with other factors. P ≤ 0.05 was considered statistically significant.
2.2. Ethical Considerations
This study was reviewed and approved by the Faculty of Medicine Research Ethical Committee, and a waiver of the consent form was approved. We used an anonymous questionnaire with no private or sensitive information. Before distributing the questionnaire, the researcher informed the participants about the objectives of the study, and the confidentiality of their information. Verbal consent was obtained prior to participation. Anthropometric measurements were conducted in a private place. All participants had the right not to participate in the study.
3. RESULTS
The socio-demographic profile of the participants is given in Table 1. The participants’ age range from 16 - 60 years with a mean age of 32.97 ± 10.72 years with a domination of female gender distribution across male as (58.8% females and 41.2% males). They urban residency was 55.8% and 52.8% were a high educated participant and occupation was almost equally distributed between the categories (professional, administrative, student and no work).
Awareness of participants about their own weight, height, Body Mass index (BMI) and waist circumference (WC): the results shown in Table 2 revealed that more than half of the participants knew their weight and height (56.0%; 50.9% respectively). Only (42.1%; 26.5% respectively) knew about (BMI) and (WC) as an indicator

Table 1. Socio-demographic characteristics of the participants.
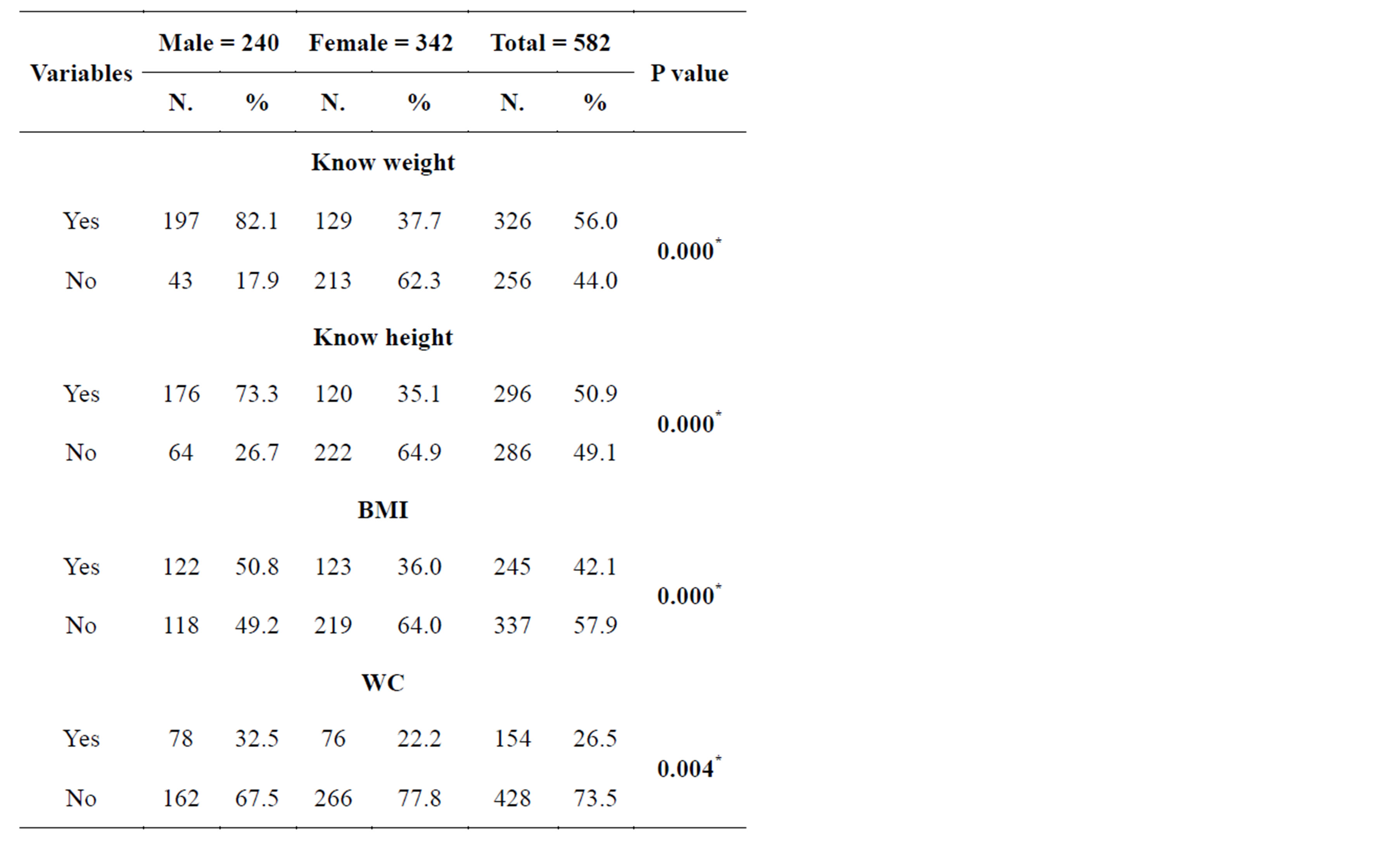
Table 2. Participants awareness about knowing weight, height, BMI and WC.
of obesity. There was a difference in awareness about body measurement as males were more aware about their body measurement than females with a highly statistical significant difference between them (P = 0.000, 0.000, 0.000, 0.004). As regards the relation between knowing weight and accurate weight numbers only 152 (46.6%) are known their accurate weight with a significant statistical difference (P = 0.000) and from (296) participants documented that they know their height, only 100 (33.8%) reported the accurate height with a significant statistical difference between them (P = 0.000).
Table 3 showed that the prevalence of obesity was (88.7%) by the BMI measure which is in contrast with the participant self-image as only (49%) of them see themselves as obese, and (13.4%) see themselves as underweight. Regarding the relation between BMI and waist circumference 156 (30.2%) of the obese participants were at risk for different diseases as their waist circumference was above the normal average Awareness of participants about their body image: the results shown in Table 4 revealed that there was a statistically significant difference (P = 0.000) between body image and the BMI. As (87.7%) of the participants selfreported as normal was obese by the BMI, and (65.4% of the self-reported underweight is considered obese by the BMI.
Table 5 revealed that there were no significant association noted between the body self-image and age categories, residency, educational status, occupation with a (P value = 0.751, 0.537, 0.192, 0.788) respectively.
Regarding the different gender in the study population, a significant association was found between them as
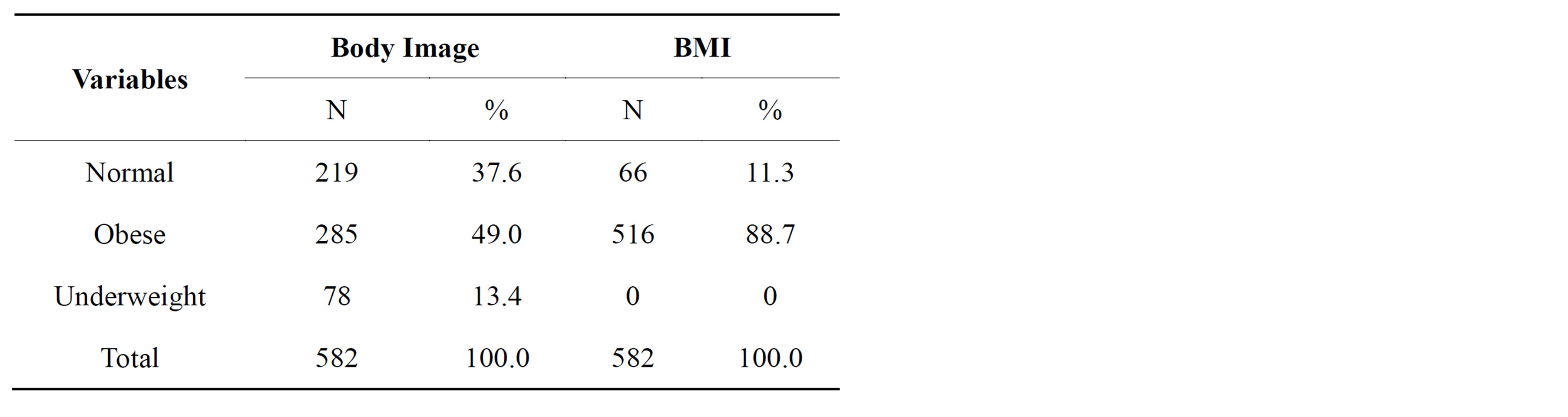
Table 3. Comparison between personal body image and BMI.
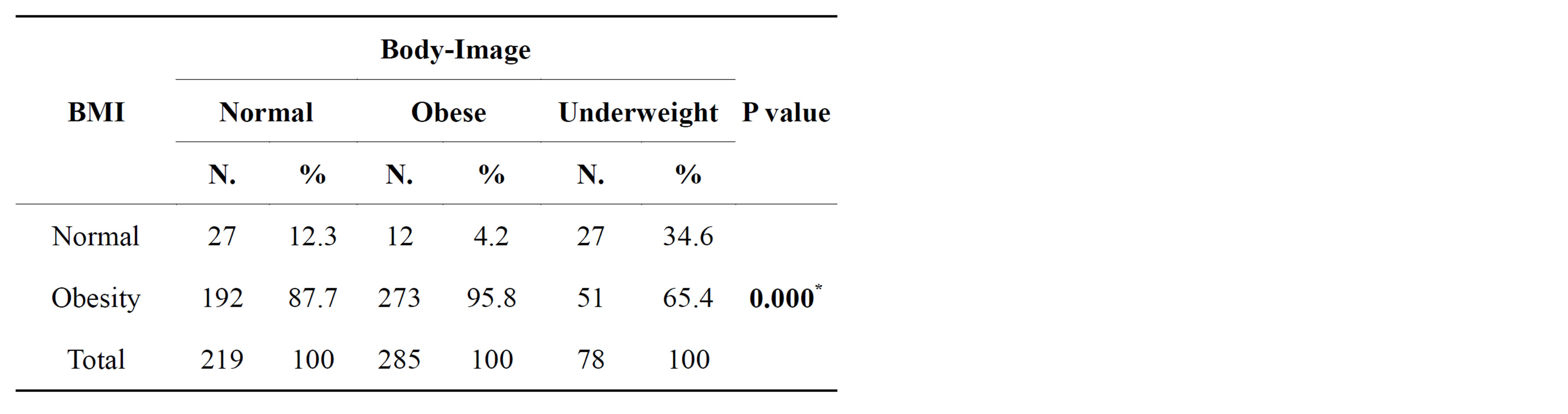
Table 4. Relation between Self-image and BMI.
knowing their accurate weight, height (P = 0.000, 0.000). Also there were a statistical significant difference of BMI and WC (P = 0.027 and 0.000) respectively. However there was no association between male and female regarding body self-image (P = 0.582) as shown in Table 6.
4. DISCUSSION
Obesity is now described as an epidemic and considered to be a major public health problem [16]. The prevalence of obesity in United States continues to be high; more than 35% of U.S. men and women were obese in 2009-2010 [17]. The WHO estimates that currently around one in every three of the world’s adults is overweight, while nearly one in every ten is obese. With nearly 70% of its adult population overweight or obese [18].
Our study was conducted in Fayoum districts and concerns 582 participants with a mean age was 32.97 ± 10.72 years and female was (58.8%) and (41.2%) males and they were nearly equally distributed between urban and rural areas with a 52.8% were a higher educated participants Table 1. Regarding participants awareness about their own weight, height, and knowing the (BMI) and (WC) as an indicators for estimation of obesity: our
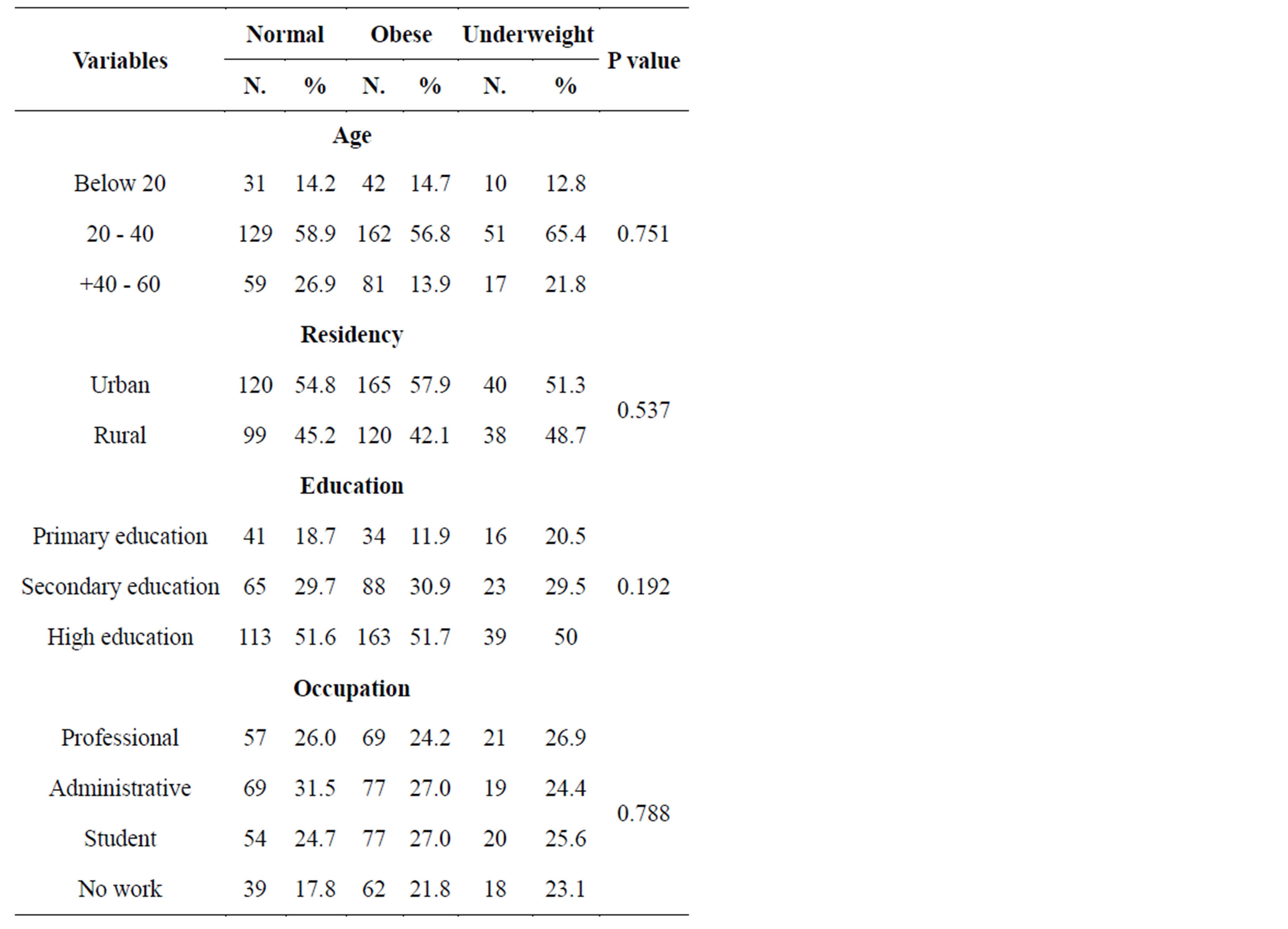
Table 5. Relation between Body image and demographic factors.

Table 6. Sex distribution regarding accurate weight, height, BMI and WC.
results shown in Table 2 revealed that more than half of the participants knew their weight and height (56.0%; 50.9% respectively) and (42.1%; 26.5% respectively) knew about (BMI) and (WC) with a highly statistical significant difference between different gender as (P = 0.000, 0.000, 0.000, 0.004) this is explained as 73% of the participants were below the age of 40 and more than half of the participants were highly educated so they were interested by knowing their weight and height and caring about their self-image. In contrast to the modern Western cultural and popular media which pressure on women to be thin, Fayoum culture preferring the overweight woman this is mainly referred to their agriculture community, that they need woman with a good body building to help them in work and be able to caring about their kids and house work. There was a statistical significant difference between knowing weight and height, and their accurate results (P = 0.000).
Virginia et al., (2003) [19] reported that although selfperception of weight status appeared highly sensitive to small changes in BMI, a large percentage of men (29.8%) and women (27.5%) placed themselves in a weight category that is incongruent with public health classifications. With respect to self-perceived weight status, most women were in the “overweight” category (62.3%), while most men were in the “about the right weight” category (48.9%). This result was in agreement with our study results as (87.7%) of the participants self-reported as normal was obese by the BMI, and (65.4% of the self-reported underweight is considered obese by the BMI. However, there was no association between male and female regarding body self-image (P = 0.582) Table 4 [20,21].
The overall prevalence of obesity in our study was (88.7%) higher in female (90.9%) than male (85.4%) Table 6 which is in agreement with the WHO report (2013) and (James et al., 2004) [2,4] that documented a higher prevalence of obesity among adult women, while overweight is more marked among adult men. This is because of major changes in life style in the past few decades [22]. In Egypt, rising obesity rates are connected to a growing number of “junk food” and fast food outlets, coupled with increasingly sedentary lifestyles.
The problem of obesity is inherently complex, and no single strategy has been determined most effective. Obesity should be addressed through a comprehensive approach across multiple settings and sectors that can change individual nutrition and physical activity behaviors and the environments and policies that affect these behaviors [23]. Changes might include: Instituting new programs, policies, and practices, changing community attitudes, beliefs, or social norms [12].
Health awareness turned out an essential mediator, which helps to promote a weight-stabilizing life-style. In order to raise health awareness; and motivate people at risk to undergo a life-style modification. There is a need for health education activity regarding obesity and its risk factors to promote healthy life style among community. Target groups should be informed about the better health status in normal weight compared with that in overweight and obese people. The mission of the Healthy People 2020 strives to increase public awareness and understanding of the determinants of health, disease, and disability, and the opportunities for progress [24].
5. CONCLUSION & RECOMMENDATION
It was clear that the prevalence of obesity in Fayoum population was high (88.7%). Also there was incorrect self-image about obesity regarding both male and female. These findings are important for public health interventions in obesity care. Public awareness about obesity, its risk factors and complication is an important determinant, and awareness needs to be increased. Implementation of health promotion and health education in the community should use effective nutrition education and incorporating positive messages in the mass-media programs to raise awareness of appropriate body weight to combat the growing level of obesity.
ABBREVIATION LIST
WHO: World Health Organization BMI: Body Mass Index WC: Waist Circumference IOTF: The International Obesity Task Force CAPMAS: Central Agency for Public Mobilization and Statistics SPSS: Statistical Package for Social Science