Received 16 November 2015; accepted 15 January 2016; published 18 January 2016

1. Introduction
The most frequent benign tumor of the heart is myxomas and accounting in approximately 30% of all primary cardiac tumors [1] . 75% are located in the left atrium [2] . Myxoma is a benign polypoid neoplasm, usually originates from endocardial cells in the region of fossa ovalis and is attached to the interatrial septum. Myxomas are pedunculated, friable and appear as a soft, gelatinous, mucoid, usually gray-white mass often with areas of haemorrhage or thrombi. They are slowly growing and usually do not produce symptoms or signs until they enlarge. Their size, shape and texture can be quite varied. Myxomas may be smooth surfaced but are more often irregularly shaped or have the appearance of a “cluster of grapes”. They are typically nonhomogeneous in texture with lucent centers or areas of calcification. Myxomas can be quite large, occupying most of the left atrium and resulting obstruction to left ventricular filling. The diagnosis can be established by the demonstration of a characteristic echo producing mass in the left atrium by two-dimensional (2D) echocardiography [3] [4] . Although asymptomatic patients with myxomas have been reported, most present with one or more effects of a triad of constitutional, embolic and obstructive manifestations [5] . Typically, these large pedunculated tumors advance through and obstruct the atrioventricular valves during diastole and are expelled retrogradely into the atrium during systole. The most common clinical presentation mimics that of mitral valve disease [6] ―either stenosis due to tumor prolapse into mitral orifice or regurgitation due to tumor induced valve trauma.
An asymptomatic large myxoma in the left atrium in an elderly is rare and so this case has been reported.
2. Case Report
A 75-year-old woman was admitted with exertional dyspnea and palpitations for the past 6 months. The patient developed the symptoms especially in sitting posture when raising from the bed in the early morning hours and get relieved when lying down. The symptoms were intermittent for a short period recently Constitutional symptoms such as arthralgia, myalgia, and weight loss were also present. Blood chemistry showed elevated erythrocyte sedimentation rate and platelets were within normal range. Pulse was irregular (112 bpm) and blood pressure was 140/90 mmHg. Symptoms and physical findings were often “positional”. Physical examination revealed mild clubbing and auscultatory findings were consistent with mitral valve stenosis and insufficiency. A loud first heart sound, low pitched “tumor plop”, a holosystolic murmur that was loudest at the apex and resembled mitral regurgitation and a mid diastolic murmur well noticed in the sitting position were the characteristic findings masquerading as Rheumatic mitral stenosis and regurgitation. ECG revealed atrial fibrillation. X-ray chest revealed cardiomegaly. Echocardiography revealed a large myxoma occupying in the left atrium, producing mitral valve obstruction as shown in the Images 1-4.
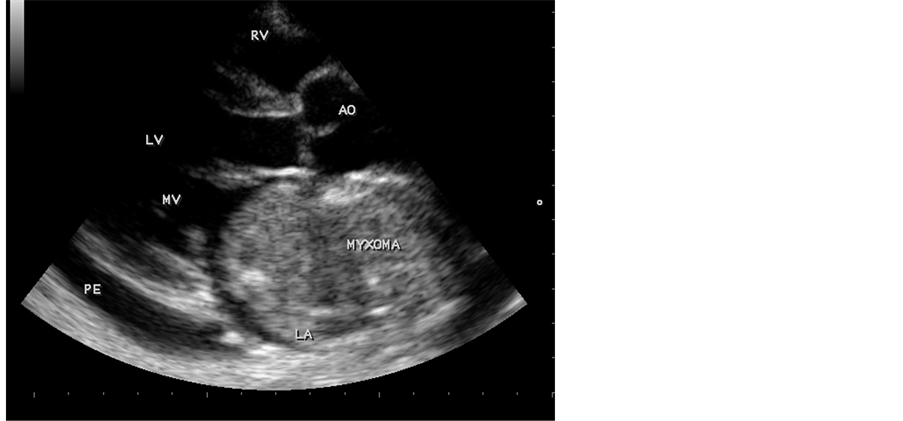
Image 1. Parasternal long axis view showing myxoma in the left atrium.
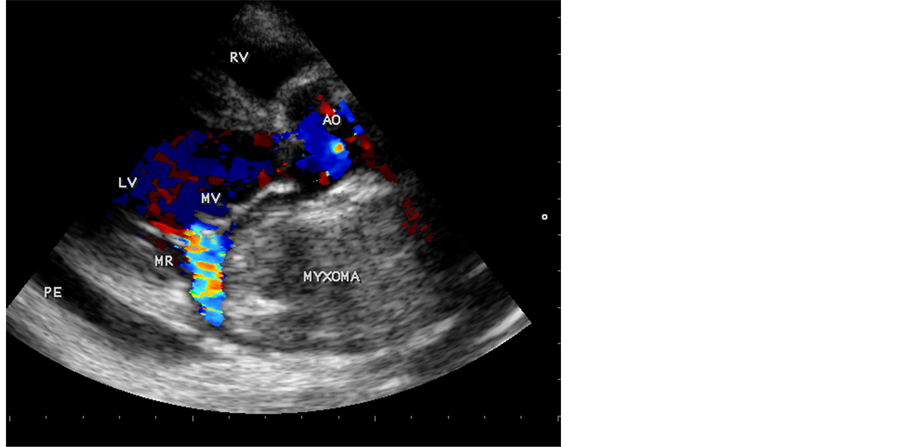
Image 2. Parasternal long axis view showing functional mitral regurgitation.
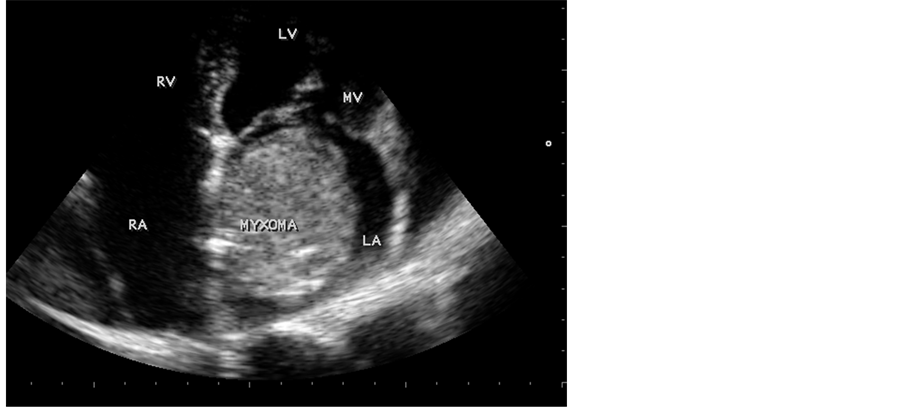
Image 3. Apical view showing the myxoma in the left atrium.
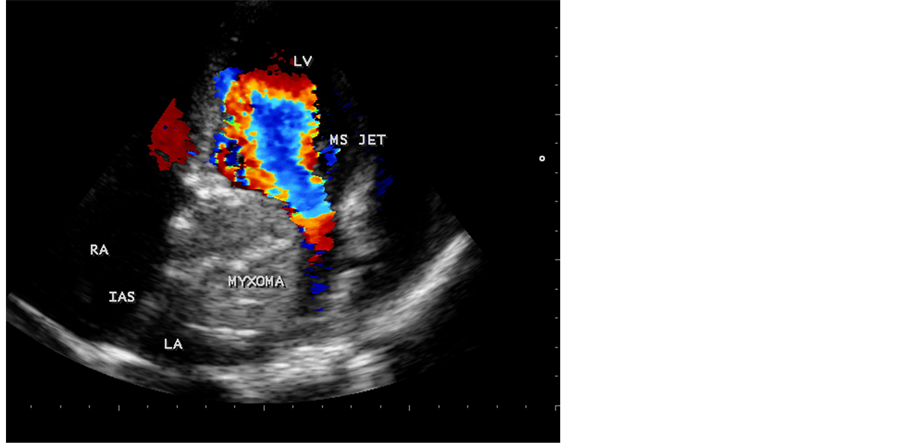
Image 4. Apical view showing the functional mitral stenosis jet.
She was given symptomatic treatment with small doses of diuretics and beta blockers such as propranolol, symptom free thereafter and advised to avoid exertion. Since the age was advanced and well maintaining basic life style, surgical intervention was not preferred in this patient.
She was followed up to two years and no further adverse events noticed in her life style. Echocardiographic screening of family members revealed no abnormality.
3. Discussion
The most common primary cardiac tumor presenting in the left atrium is the benign myxoma, which in the large majority of cases is solitary [7] . In a large single-Institution series of primary cardiac tumors, 42% were cardiac myxomas [8] . The proportion of myxomas in comparison with other tumors was increased to 77%. The mean age of presentation with sporadic myxoma is 56 years and 70% are females in the age group of 3 to 83 years. The cause of syndrome myxoma is unknown [9] . It has been proposed to result from a widespread abnormality resulting in excessive proliferation of certain mesenchymal cells and excessive glycosaminoglycans production by them. Most tumors are histologically benign and potentially lethal due to intracavity or valvular obstruction, peripheral embolism and conduction disturbances. The association of constitutional symptoms is likely due to synthesis and secretion of interleukin-6.
Left atrial myxomas prolapse to various degrees into mitral valve orifice, resulting in obstruction to AV (atrioventricular) blood flow and frequently, mitral regurgitation. The resultant signs and symptoms often mimic those of mitral valve disease [10] , especially mitral stenosis. Symptoms of sudden in onset, intermittent and related to the patient’s body position [11] should raise the suspicion of left atrial myxoma. When atrial myxomas obstruct the AV valves, the patient may experience dyspnea, dizziness or syncope when sitting or standing with alleviation of symptoms on lying down. Sudden death may also occur. The loud first heart sound that occurs in patients with left atrial myxoma may be due to the late onset of mitral valve closure resulting from prolapse of the tumor through the mitral valve and frequently split, with the second component corresponding to the expulsion of the tumor from the mitral orifice. In many cases, an early diastolic sound, termed a “tumor plop” can be identified and it is thought to be produced as the tumor strikes the endothelial wall or its excursion is abruptly halted. If the obstruction is incomplete, the tumor plop may be followed by a diastolic rumble. When the obstruction becomes more severe, cardiac output may fall precipitously.
Given a typical presentation, Echocardiography is virtually diagnostic of myxoma. The ability to detect atrial myxoma of the heart by means of echocardiography was first reported more than two decades ago by Effert and Domanig. 2D echocardiography is the non invasive procedure of choice for the diagnosis of left atrial myxoma. The virtual pathognomonic finding of an atrial myxoma is that of a large pedunculated tumor mass traversing through the AV valves in a to-and-fro motion. Large atrial myxomas have been classified by echo appearance as follows [12] .
Class I-small and prolapse through the mitral valve.
Class II-small and non prolapsing.
Class III-large and prolapsing.
Class IV-large and non prolapsing.
Myxomas are mottled in appearance and in some atrial myxomas, areas of echolucency corresponding to areas of haemorrhage within the tumor which are not seen in thrombi or infective lesions. In this case, 2D echocardiographic Image 1 and Image 3 illustrate the myxoma in the left atrium (size 54.8 × 45.6 mm) and Colour Doppler Image 2 and Image 4 illustrate its obstructive features masquerading as Rheumatic mitral regurgitation and stenosis. Echocardiographically, the mitral valve appears as normal without any evidence suggestive of Rheumatic process such as commissural fusion, valve thickening and calcification. The resultant mitral stenosis and regurgitation are due to the movement of the myxoma across the mitral valve and so they are functional, masquerading as Rheumatic mitral stenosis and regurgitation in this case.
Surgical excision is the treatment of choice for most benign cardiac tumors and in many cases results in a complete cure. Recurrence is 1% to 5% after resection. Large size of myxoma together with location on posterior left atrial wall necessitates complete removal of the heart which was followed by “auto transplantation” i.e., reimplantation of the patient’s excised heart.
4. Conclusion
A large myxoma occupying in the left atrium remains asymptomatic up to the age of 75 years in a female is a rarest presentation in tropical countries such as India at Thoothukudi coastal region in Tamil Nadu State.