Predictors of Successful Weight Loss Maintenance: A Qualitative Comparative Analysis ()
1. Introduction
Obesity and related diseases place a huge financial burden on the country, costing approximately 10% of total medical spending in 2008 [1] . Weight loss (WL) attempts, particularly utilizing behavioral lifestyle methods, are largely successful [2] ; however, maintaining WL is challenging for most people, and relapse is common [3] [4] . The majority of those successful at WL regain all lost weight within 3 - 5 years after treatment [5] - [7] . The like- lihood of continued success increases for those who are able to maintain their initial WL for ≥2 years [8] [9] . Identifying practical, sustainable solutions for effective WL and weight loss maintenance (WTLM) that can be implemented at the clinical practitioner level are essential [4] [10] .
Changing lifestyle behaviors remains at the forefront of effective WTLM treatment strategies. Self-monitor- ing of body weight, physical activity, and fruit and vegetable consumption are effective WTLM behaviors [11] [12] , and increasing water intake may be an important strategy as well [13] [14] . However, individuals success- ful at WTLM implement behavior changes in varying amounts and combinations [15] . Weight loss in response to habitual physical activity and dietary intake exhibits a wide inter-individual variability, and thus, despite sim- ilar amounts of physical activity or patterns of dietary intake, some individuals may not achieve successful WTLM [16] . This individual variability in behavior implementation and weight change responses has led re- searchers to attempt to identify specific predictors of successful WTLM in order to develop more effective WTLM strategies.
Behavioral and physiological evidences suggest that sex may be an important predictor of WTLM success. A long-standing notion that men are more successful at WL and WTLM with less effort than women exists among the general public and practitioners [17] , but because men are typically underrepresented in behavioral interven- tions, research comparing sex differences in WTLM is sparse [18] [19] . Physiological evidence suggests that women experience a compensatory increase in energy intake in response to physical activity, which may thwart efforts to maintain WL through physical activity, whereas men do not [20] [21] . Other research indicates that men more accurately regulate energy intake in an acute ad libitum meal after a calorie-containing preload [22] . Because many physiological functions influence behavioral processes [23] , men and women likely approach WTLM with differing behaviors. Through structural equation modeling, Wang et al. found that though men and women have a similar mediator (i.e., attention to weight and health habits) in predicting health behavior out- comes (i.e., eating behavior, eating out behavior, and physical activity), the moderating effect of predictors on the relationship between the mediator and health behavior outcomes is more complex for women than for men [24] .
Within this context, the overall purpose of this investigation was to observe the occurrences of weight relapse (i.e., ≥3 lb weight gain) and describe behavior changes in response to weight change. Additional objectives were to determine if sex differences exist in maintenance of clinically significant WL and to determine if there were differences in the interaction of sex and WTLM behaviors, specifically in reported fruit and vegetable intake and physical activity.
2. Methods
2.1. Subjects and Design
This investigation was a retrospective analysis of data collected from two previously conducted intervention tri- als of WL and WTLM, the details of which have been described previously [25] [26] . Study protocols for both intervention trials were approved by the Virginia Tech Institutional Review Board, and all participants provided written informed consent prior to enrollment in the studies [25] [26] . Briefly, individuals aged 55 - 75 years were invited to participate in a single-blind randomized controlled trial, led by a registered dietitian, in which they were assigned to one of two WL groups for 12 weeks: a) 1200 to 1500 kcal hypocaloric diet or b) 1200 to 1500 kcal hypocaloric diet + 16 fl oz water prior to each main meal [25] . Because the number of obese mid- dle-aged and older adults has increased in recent years, addressing strategies for WL and WTLM in this popula- tion is warranted [26] . Following the WL trial, participants were invited to enroll in the WTLM trial [26] . Of the 42 individuals who completed the WL trial, 39 completed the WTLM trial [26] . Individuals continued within their WL trial randomization group (i.e., 16 fl oz water preload or no water preload) but without caloric restric- tion and were asked to self-monitor their daily body weight, physical activity (measured by pedometer step count), and fruit and vegetable intake (measured by servings). Participants in the water preload group were asked to also self-monitor their water consumption [26] . All participants were provided tracking sheets to record their daily behaviors and were asked to return tracking sheets weekly to the study coordinator [26] . Overall pro- gram goals for all participants were to maintain their reduced body weight (within 3 lbs of their laboratory- measured baseline body weight), achieve 10,000 or more steps per day, consume at least 5 servings of fruits and vegetables daily, and, for the water preload group only, consume at least 48 fl oz of water each day [26] . Partic- ipants were considered compliant with returning tracking sheets regardless of accuracy or completeness. Body weight, blood pressure, and four day food records were assessed monthly in the laboratory. Body composition (DXA) (GE Lunar Prodigy; GE Healthcare, Madison, WI) and resting metabolic rate (RMR) via indirect calo- rimetry (Parvo Medics TruOne 2400, Sandy, UT) were evaluated at baseline, 6, and 12 months of WTLM [26] . For the purposes of this post hoc analysis, groups were primarily distinguished by sex, rather than the original randomization to water preload or no water preload groups, although original group assignment was included in the statistical and qualitative analyses. Successful WTLM was defined as remaining below or within 3 lbs of baseline-measured body weight.
2.2. Qualitative Analysis: Predictors of Weight Loss Maintenance Success
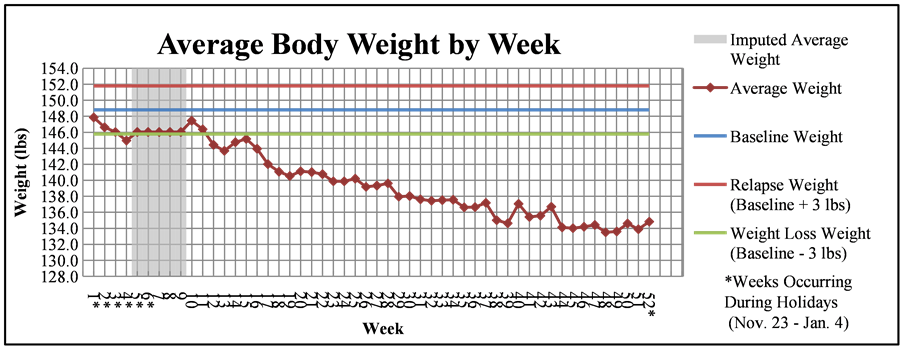
Single missing values for daily body weights were replaced using the mean of nearby points in the Statistical Package for the Social Sciences software (SPSS, version 20.0 for Windows, 2011, SPSS Inc., Chicago, IL), and missing daily values for behaviors (physical activity, fruit and vegetable intake, and water consumption) were imputed using the expectation-maximization algorithm. The expectation-maximization method first determines a conditional expectation for a missing value based on observed values and then uses maximum likelihood esti- mates of parameters to find the most likely value [27] . Because of the high daily variance of behavioral data, in contrast to the relatively consistent daily body weight measurements, the expectation-maximization algorithm was used rather than calculating the mean of surrounding data points. Once missing values were replaced, weekly averages of body weight, exercise, fruit and vegetable intake, and water consumption (for the water preload group only) were calculated. Graphs illustrating changes in weekly averages of these variables for each participant were generated.
The 39 individual graphs were then categorized based on weight outcomes (i.e., successful or unsuccessful, in terms of a 3 lb regain). Participants were characterized using the following four discrete weight change catego- ries: WL (n = 13), weight stable (n = 7), relapse with recovery (n = 9), and relapse without recovery (n = 10). WL participants were defined as those who lost weight over the course of the 12-month period and whose aver- age final week remained ≥3 lbs below baseline weight. Weight stable participants remained within 3 lbs of base- line weight and never exceeded a 3 lb gain from baseline. Those in the relapse with recovery group gained ≥3 lbs more than baseline body weight at least once during the study period but recovered to within 3 lbs of base- line weight by the final week’s average weight. The relapse without recovery group consisted of individuals who gained ≥3 lbs more than baseline weight at least once during the study period and remained ≥3 lbs above base- line weight during the final week. Figure 1 depicts examples of individual graphs for each of the four weight outcome groups.
Once graphs were categorized, three researchers then independently reviewed individual graphs within each category and discussed observations. Individuals who were noncompliant in returning tracking sheets for weeks 45 - 52 consecutively were excluded from further analysis (n = 10) based on the reasoning that imputed average weights and behaviors for the final weeks could potentially categorize an individual incorrectly. Individual cha- racteristics related to weight and behavior change were assessed and observations were discussed among re- searchers.
Based on these general observations, a crisp set qualitative comparative analysis (QCA) was used to deter- mine behavioral conditions and factors required for the desired outcome (i.e., successful WTLM) to occur. QCA is a tool used in exploratory evaluation to probe for potential preliminary information with combined qualitative and quantitative techniques [28] . In this type of analysis, conditions potentially associated with a given outcome are calibrated in a dichotomous manner to identify multiple causations of an outcome while still maintaining the heterogeneity of individual characteristics [28] . Conditions deemed “necessary” are present in all successful categories but may also be present in unsuccessful ones, and “sufficient” conditions or combinations of condi- tions are present only in successful categories and must be present for the desired outcome to occur [28] . For the QCA, researchers determined a list of potentially causal conditions and defined decision rules for each condition.
Data were then dichotomously calibrated for each condition based on the specifically defined rules, and re- sults were documented in a truth table. Causal conditions were assessed for weight outcome groups and by sex.
2.3. Statistical Methods
Statistical analyses were performed with SPSS. Baseline characteristics for men and women were assessed using independent samples t-tests and descriptive statistics. Sex difference in clinically significant WL at 12 months of the WTLM trial was analyzed with Pearson’s Chi-squared test, using the criterion of ≥5% total WL, from base- line of the WL trial. A 5% - 10% WL in obese patients is associated with reductions in mortality and risk factors for cardiovascular disease and type 2 diabetes [29] , and therefore, maintenance of even modest WL would provide important health benefits for most reduced-obese individuals. To assess potential interactions of sex and behavioral predictors of WTLM, a random coefficients (mixed) model (i.e., growth curve analysis) was used because it is able to correct for measurement unreliability and uses individual trajectories to measure change rather than averages [30] . Due to the high variance in daily reported physical activity, log-transformed physical activity was used in the model. Because of the limited sample size, separate growth curve models with bootstrapped standard errors were estimated for the 0 - 6 month and 7 - 11 month time frames.
3. Results
The sample was 93% white, and 43% were men. Overall, the mean age was 62.7 ± 5.9 years, and the mean BMI was 29.3 ± 4.8 kg/m2. There were no significant differences between sexes at baseline in age, BMI, or prior per- cent WL (all >0.05).
3.1. Qualitative Analysis of Weight Relapse
Table 1 presents the raw data of the QCA results by weight outcome groups. In the truth table, present condi- tions are denoted by “1,” and conditions not present are denoted by “0”.
The QCA for the full sample revealed four conditions considered necessary for successful WTLM overall: 1) adherence to at least one behavioral goal, 2) adherence to the fruit and vegetable intake goal, 3) adherence to the water intake goal, and 4) occurrence of weight gain during the holidays. No two weight outcome groups shared the same pattern of conditions overall. Interestingly, the condition of early first relapse was found to be a neces- sary and sufficient condition for failure of WTLM. That is, if an individual gained ≥3 lbs during the first 13 weeks of the intervention, he or she was guaranteed to fail at WTLM. Overall, continued WL at 12 weeks and a maximum WL of ≥5 lbs from WTLM baseline body weight as a combination of conditions were sufficient for the WL outcome at 12 months.
![]()
Table 1. Qualitative comparative analysis results with four weight outcome groups presented as a truth table.
Conditions present are designated by “1,” and conditions not present are designated by “0”. WL = weight loss; FV = fruit and vegetable intake; PA = physical activity.
In general, participants categorized in the WL group were adherent to the fruit and vegetable intake goal but did not exceed the goal on average throughout the study. Additionally, they continued to lose weight through the first three months and achieved ≥5 lb WL overall (measured from WTLM baseline body weight). Weight stable individuals exceeded at least one behavioral goal, either the fruit and vegetable intake goal or the water goal, and experienced weight gain during the holidays. While some lost weight throughout the study period, particu- larly during the first three months, the weight stable group on average never lost ≥5 lbs. In general, the relapse with recovery group exceeded at least one behavioral goal. Women in the group were typically adherent to the fruit and vegetable goal and exceeded the water intake goal, while some men additionally exceeded the physical activity goal. Among the relapse without recovery group, early first relapse and holiday weight gain were nota- ble conditions. Adherence to at least one behavioral goal was also exhibited by individuals in the relapse without recovery group.
Weight outcome groups are divided by sex in Table 2. Only for men in the WL group was holiday weight gain not a necessary condition; for all other sex and outcome group categories, weight gain during the holidays was present. Men in both the relapse with recovery and relapse without recovery groups were adherent to at least two behavioral goals, but this condition was not present in any outcome group for women.
3.2. Sex Differences in Clinically Significant Weight Loss and Weight Loss Maintenance Behaviors
Potential physiological predictors, including resting metabolic rate per kg of fat free mass (RMR per kg FFM) and percent body fat measured at baseline, 6, and 12 months, were not included in the growth curve model be- cause no sex differences (all p > 0.05) were found in these variables during preliminary analyses. Overall RMR per kg FFM and percent body fat have been reported previously [26] . There was no significant sex difference in achieving clinically significant WL (≥5% WL) at 12 months (Χ2 = 0.123, p = 0.73). Figure 2(a) depicts the growth curve model with 0 - 12 months, and Figure 2(b) and Figure 2(c) highlight the growth curve models with 0 - 6 months and 7 - 11 months, respectively. In the overall growth curve model, the sex difference in
![]()
Table 2. Qualitative comparative analysis results comparing men and women within four weight outcome groups presented as a truth table.
Conditions present are designated by “1,” and conditions not present are designated by “0”. WL = weight loss; FV = fruit and vegetable intake; PA = physical activity.
weight change was not statistically significant (p = 0.85). Visual inspection of the growth curve model indicates potential differences in weight change between men and women during months 1, 4 - 6, and 10 - 12 may be present. However, no significant difference was found when the growth curve models were run separately by the two time frames, possibly due to limited statistical power.
4. Discussion
The primary finding of the present study was that no significant sex difference in weight change over time was observed; however, there were several important observations from the QCA. The key to WTLM success was evident in the first three months of the intervention. Those who were successful, even despite relapse, continued to lose weight in the first three months of WTLM. This may have allowed them to create a weight “buffer” to prevent excessive, irrecoverable weight gain. In contrast, individuals who failed at overall WTLM, despite ef- forts to recover (i.e., increasing engagement in behaviors), experienced relapse early in the intervention (within ~three months). These findings are in agreement with findings from the National Weight Control Registry, which found that few participants recover from even small (1 - 2 kg) amounts of weight regain and that pre- venting large regains from occurring early during WTLM is vital to recovering from relapses that occur later in WTLM [31] . From these findings, it appears that WTLM success at 12 months may be dictated by the patterns of weight change early during WTLM; therefore, the initial weeks of WTLM treatment are likely a “high-risk” period that requires more vigilant efforts in behavior modification to ensure future success.
Furthermore, the WL outcome group was the largest (n = 10), suggesting that perhaps personal WL goals had not yet been achieved at the onset of the WTLM trial. These findings are consistent with previous work sug- gesting that maximum WL is typically achieved by approximately six months of treatment [3] . In addition, indi- viduals who lose more weight early on during WL treatment may sustain WTLM success longer than those who
![]()
![]()
![]()
Figure 2. (a) Body weight change according to monthly labora- tory body weight measurements for 12 months among men and women, (b) Body weight change estimations with bootstrapped standard errors for 0 - 6 months among men and women, and (c) Body weight change estimations with bootstrapped standard er- rors for 7 - 11 months among men and women. Equations used for the overall model and estimations with bootstrapped standard errors for 0 - 6 months and 7 - 11 months are shown.
lose weight more gradually [3] . Thus, more intensive WL treatments lasting at least six months to maximize WL coupled with vigilant weight and behavior monitoring during the transition from WL to WTLM may enhance long-term WTLM success.
Holiday weight gain is common in most individuals attempting WTLM, which is consistent with other reports [32] . Although some amount of weight gain during the holiday period is likely, holiday weight gain in this sam- ple did not affect WTLM outcomes nor relate to irrecoverable relapse. Adherence to the physical activity goal was not found to be a sufficient or necessary condition for WTLM success; this finding is in contrast to exten- sive data acknowledging physical activity as a principal behavior among individuals successful at WTLM and a potential predictor of success [33] -[36] . It may be that individuals did increase engagement in physical activity compared to baseline amounts, but they may not have been able to meet the 10,000 steps/day goal established by the study investigators and, thus, were considered non-adherent.
The analytic approach used in the present study possesses several unique strengths. First, it utilized individu- als who were highly successful overall at WTLM (i.e., 80% success rate at 12 months) when compared to simi- lar clinical WTLM interventions across the field. Wing and Phelan [31] noted an approximately 20% success rate at WTLM across studies, when success is defined as maintaining ≥10% WL for ≥1 year. Second, the WL trial produced similar relative WL results in men and women (−7.78% ± 0.82% and −7.05% ± 0.78%, respec- tively); thus, both men and women began the WTLM trial with nearly the same reductions in body weight. Third, 17 out of 39 individuals in the WTLM sample were men, a proportion much higher than found in most beha- vioral interventions, and therefore, comparisons between sexes could be made. Fourth, 12 months of daily self- reported body weight, physical activity, fruit and vegetable intake, and water intake for each individual were available for qualitative analysis of the inter-individual variability in behavior change surrounding weight change.
There are several limitations within this analysis. First, the duration of the study does not permit conclusions to be drawn about WTLM beyond one year. Although self-reported daily body weight was used, self-monitored weights were highly correlated with monthly body weights measured in laboratory assessments (r = 0.99, p < 0.001). Finally, the small sample size is a limitation, but the qualitative analysis of individual data for a full 365-day study period is a unique approach providing useful information for those interested in designing larger- scale trials of WTLM.
5. Conclusion
In summary, sex differences in weight change or total WL outcomes were not observed in the present analysis. However, the results of our study suggest that men and women may approach WTLM with different behaviors. Further research to identify predictors of successful WTLM, particularly pretreatment factors (including sex), is essential to determine appropriate WTLM treatment strategies for an individualized approach. In current prac- tice, intensive WL treatment lasting at least six months should be used to maximize initial WL, and concerted effort should be made during the transition period from WL to WTLM to vigilantly monitor weight to prevent large, early weight regains, which can sabotage future WTLM success. Additionally, WTLM treatment pro- grams should implement the concept of individualized treatment in current practice, even though research has not determined all factors predicting success, and should focus on autonomy and flexibility in treatment strate- gies to match individuals’ preferences with treatment characteristics.
NOTES
*Corresponding author.