Pulmonary metastasis from gastric cancer: A case report and review of literature ()
1. INTRODUCTION
Gastric cancers are associated with a higher incidence of liver metastasis, which has a low radical resectability rate. Even without disseminated or multiple liver metastasis, pulmonary metastasis typically has carcinomatous lymphangitis or carcinomatous pleuritis. In contrast, nodular lesions are rare. Surgical resection is therefore usually not indicated. We herein describe a patient with proven pulmonary metastasis of gastric carcinoma 18- year-after total gastrectomy.
2. CLINICAL SUMMARY
A 45-year-old male underwent a total gastrectomy for gastric cancer in July 1994 (Figure 1(A)). He had no history of drinking or smoking, and his past medical and family histories were unremarkable. Histological examination revealed a poorly differentiated adenocarcinoma, which was classified as pT2 (MP) N0M0, stage II. Blood chemistry analyses were unremarkable, and tumor markers (i.e., carcinoembryonic antigen and carbohydrate antigen 19 - 9) were all within normal limits. Following gastrectomy, the patient was asymptomatic and continued follow-up for 5 years at an out-patient clinic. Then he underwent a medical examination yearly.
In November 2011 (63 years old), chest X-ray revealed an approximately 1-cm nodular shadow in the left upper lung field. Chest computed tomography (CT) revealed a tumor 9 × 8 mm in size, at the subpleural portion in left S3 of the lung (Figure 1(B)). The well-defined tumor had a CT value of 60 Hounsfield Units (HU) and enhanced CT values of 210 HU after 40 seconds and 100 HU after 2 minutes. Fluorodexyglucose accumulation (maximum standardized uptake value [SUVmax] = 2.8) of was shown on fluorodexyglucose positron emission tomography (FDG-PET) (Figure 1(C)). Fiberscopic evaluation of the upper intestine and total colon found no abnormalities. Initially, we thought that the lung tumor was either primary or metastatic lung cancer. Surgery was indicated, even for pulmonary metastases, because there was no evidence of recurrence at extrapulmonary sites, such as the primary site or the liver, by FDG-PET.
The tumors in the left lung were resected thoracoscopically, and were well defined and red in color (Figure 1(D)).
Histologically, the tumor consisted of solidly grown eosinophilic polygonal cells (Figure 2(A)), and had the following immunostaining properties: cytokeratin (CK) 7-negative, TTF-1-negative and CK 20-weakly positive (Figures 2(B) and (C)). The tumor was diagnosed as poorly differentiated carcinoma, most likely metastatic adenocarcinoma, accorded with the previous gastric cancer from the pathological report.
The patient was discharged 10 days after partial resection without any unusual events. After pulmonary resec-
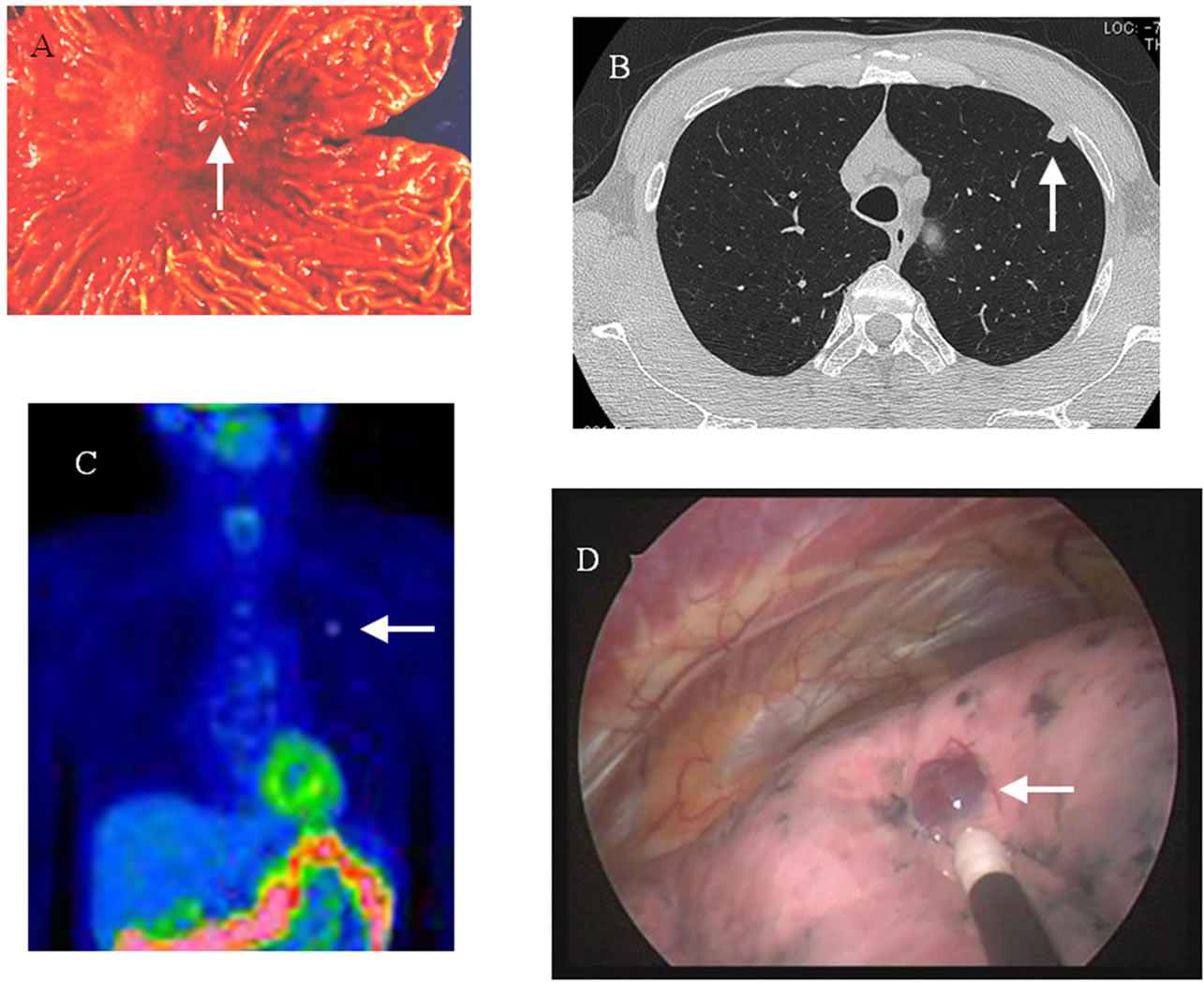
Figure 1. (A) Resected specimen of gastric cancer. (B) Chest CT showed a tumor 9 × 8 mm in size at the subpleural portion in the left S3 of the lung. The well-defined tumor had a CT value of 60 Hounsfield Units. (C) FDG accumulation was shown by PET (SUVmax = 2.8). (D) Thoracoscopic findings showed that the tumor was well defined and red in color.
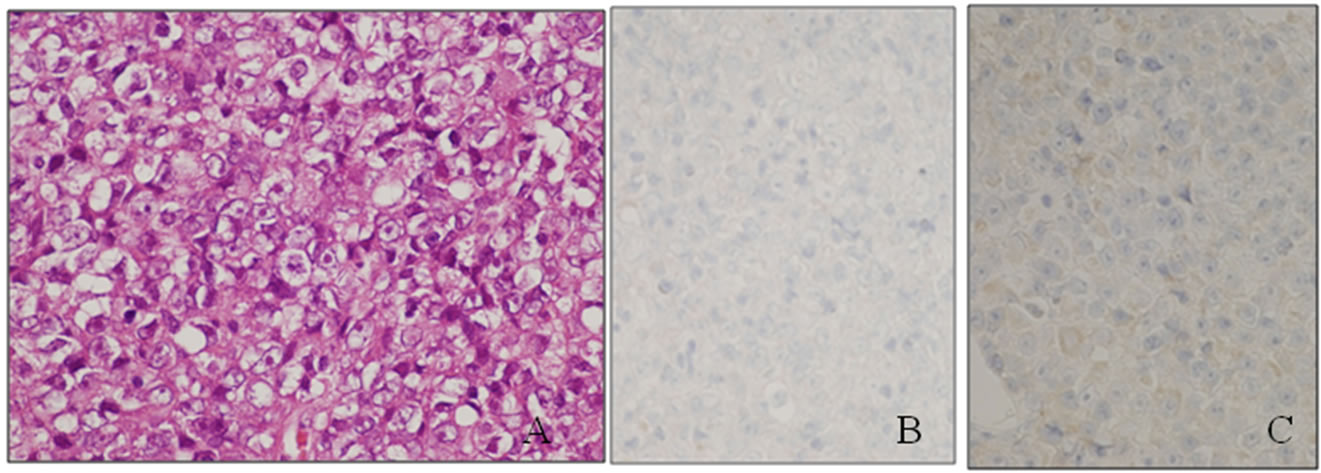
Figure 2. (A) Histological findings of poorly differentiated carcinoma of the left lung (hematoxylin and eosin staining). (B) Immunohistological findings of TTF-1 immunostaining. (C) Immunohistological findings of CK 20 immunostaining.
tion, we provided follow-up care at our out-patient clinic for 15 months. There were not new nodules on chest CT, and fiberscopic evaluation found no abnormalities in the upper intestine or total colon. Based on the clinical course and pathological-futures, we concluded that the patient had pulmonary metastasis of gastric carcinoma 18 years after total gastrectomy for gastric cancer.
3. DISCUSSION
Based on autopsy results, the incidence of pulmonary metastatic lung cancer from gastric cancer has been reported at 49.6% [1]. Surgical resection is rarely indicated for recurrent or metastatic gastric cancer because it tends to occur at multiple sites and shows aggressive biological behaviors [2]. It is reasonable to assume that the lung metastases in these case were from the stomach because there were multiple, small lung lesions, unlike the single location of their gastric neoplasm. In our case, the tumor was well defined and round and there was a subpleural portion. The tumor was not stained by TTF-1 for pulmonary tumor maker. We therefore thought that the pulmonary tumor was a metastatic lung cancer.
The patient was asymptomatic and had no recognizable neoplasm by gastrointestinal fiberscope findings, chest and abdominal CT, or FDG-PET findings between the perioperative period and 15 month follow-up. No new lesions have arisen at any pulmonary or another sites.
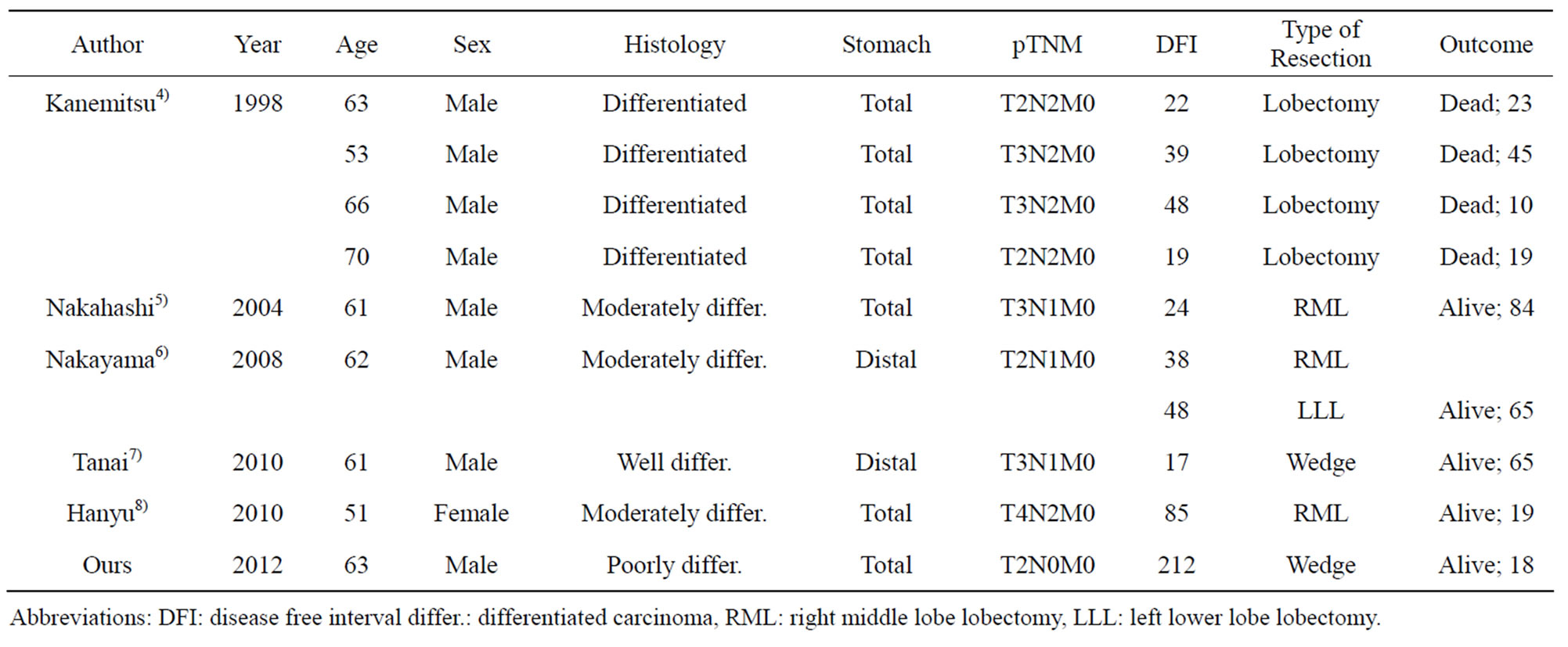
Table 1. Characteristics of cases of pulmonary metastasectomy for gastric cancer.
Abbreviations: DFI: disease free interval differ.: differentiated carcinoma, RML: right middle lobe lobectomy, LLL: left lower lobe lobectomy.
The tumors were weakly positive for CK 20, a gastrointestinal maker. A combination of TTF-1−CK20+ was highly significantly associated with adenocarcinoma of gastrointestinal origin [3]. The sensitivity and specificity of this combination of immunomarkers for a metastatic adenocarcinoma from gastrointestinal tract were 79% and 100%. He had past history of resected gastric cancer. The tumor accorded with the previous gastric cancer from the pathological report, was diagnosed as poorly differentiated carcinoma, most likely metastatic gastric adenocarcinoma.
Surgical resectable solitary metastasis only occurs in 0.1% in patients who have undergone curative resection for gastric cancer [4]. By the end of 20th century, the time interval to recurrence following pulmonary resection ranged from 6 to 36 months, all the median survival after recurrence was 24.3 months. Several cases of resection of solitary pulmonary metastasis from gastric cancer have been reported (Table 1) [4-8]. In recent years, advances in anesthesia and thoracotomy procedure have improved survival, and improvements in high-resolution CT and FDG-PET have increased detection. Carefully selected patients have good chance of successful pulmonary metastasectomy for gastric cancer.
4. CONCLUSION
In summary, we describe a case of pulmonary metastases from gastric carcinoma that was treated with surgical resection. At least empirically, surgery may be considered a treatment of choice to improve the long-term survival in such patients.