Community Knowledge and Attitude about Burns First Aid (BFA) in Jazan, Saudi Arabia ()
1. Introduction
Burn injuries are a continuous and considerable public health problem which is the fourth most common type of trauma worldwide [1] . Burn-related injuries occur when hot liquids, solids, or a flame rupture one or more of the skin’s layers. Also, “burn” is a term describing skin damage by chemicals, electricity, or radiation [2] . These injuries are a major cause of mortality and morbidity in developing countries, affecting about 11 million people worldwide with an estimated 300,000 deaths every year and contributing to morbidities like an increase in hospital stays and development of disability afterward [3] . In Saudi Arabia, burns remain a major source of injury with a prevalence of 112 to 518 per 100,000 per year particularly among young children, in whom the major mechanism of injury appears to be scalding from hot liquids [4] . Initial early management, which involves first aid measures at the scene of the burn accident before access to a hospital, and before transfer to a burns center, is a highly important step in burn management [5] .
Proper and simple initial treatment when correctly applied has the potential to reduce injury depth, pain, and post-burn complications [6] . Studies have shown that appropriate first-aid interventions reduce morbidity-related costs and tissue effects, resulting in a lower need for surgical procedures [7] . Performing first aid, stopping the burn process, and taking immediate measures like running cold tap water for at least 10 - 15 min, removing clothing and jewelry, and dressing the wound with a sterile dressing will help improve the outcomes of burns [6] . In contrast, some individuals have been utilizing a variety of topical remedies such as ice, herbal medicines, oil, honey, vinegar, flour, toothpaste, and eggs to treat burn injuries without any scientific proof [8] . Giving such odd remedies worsens the wound and encourages bacterial development, increasing the post-burn consequences [9] . So, people must have an appropriate level of knowledge for the first aid management of burn injuries to save themselves and to help others. However, inadequate public education regarding burn first aid (BFA), injury prevention, and control methods and a lack of resources in underfunded health facilities contribute to the observed poor results.
In recent years, widespread attempts to reduce the risk of burns by increasing public awareness and encouraging individuals to undertake steps like installing and maintaining fire alarms and lowering the heat of water in the home has led to an apparent decrease in burn incidence and mortality, especially in more developed countries [8] . In addition, the prompt and effective application of BFA has been shown to positively impact the burn outcome, preventing further tissue damage and reducing subsequent morbidity [10] . It was observed in a recent cohort study that 20 min of running water received as first aid had improved outcomes by about 58.1%. This intervention was associated with a statistically significant reduction in burn wound depth, faster healing (by 10%), and less need for skin grafting. Furthermore, patients who did not receive appropriate first aid had a higher complication rate (35.3% vs. 18.4%) compared with patients who received [11] . Gete et al. [12] reported in a cross-sectional study that 66.2% of respondents had poor knowledge of proper BFA. The majority (80.7%) of respondents did not take any form of BFA training. Females were almost four (4) times more likely to have good knowledge as compared to males. Also, there was a significant correlation with knowledge as seen in participants living in rural areas were almost 61% less likely to have good knowledge of BFA as compared to those living in urban areas. A significant number of participants 79 (25.9%) were still using traditional home remedies as a BFA, which has no scientific value. Wallace et al. [13] in their study showed that older males (≥65 years) age groups had relatively lower levels of BFA awareness. Also, most participants who did not take part in any training courses for BFA had significant limitations of awareness, of them, only 15% had sufficient knowledge and only 9.4% knew the practice in cooling the burn wound surface. In summary, BFA training has played an important role in the past five (5) years which increased the knowledge. Graham et al. [14] , in their study done in Southern Yorkshire, Britain found that around 73% of mothers used cooling methods on the burn wound, approximately 92% of parents applied cover to the burn wound with appropriate materials while less than 40% parents remove clothing and jewelry and 35% applied water in sufficient time. Harvey et al. [15] found in their study conducted in New South Wales that most respondents (82%) would cool a burn with water, but only 9% knew the recommended 20 minutes. Few respondents reported that they would remove the patient’s clothing and keep the injured person warm. First aid books (42%) and the internet (33%) were the most common sources of first aid information. Those over 65 years had insufficient first-aid knowledge. Cross-sectional study conducted in KSA in 2020 found that the knowledge level is not enough regarding first aid for burn patients along with the healthcare professionals. Participation in a previous burn training course was much linked to improvement in information regarding knowledge across groups of different genders, ages, and races (P < 0.001) [16] . A recent cross-sectional survey conducted in Jeddah; KSA, in July 2022 showed that the majority of participants (52.7%) had an excellent level of knowledge about BFA. A common misconception was to pick blisters (46.8%) which is an incorrect action. Interestingly, the oldest age group (>50 years) was shown to have considerably higher knowledge scores (P = 0.0001) which were in contradiction to other studies [17] .
The most important step in burn injury management that significantly affects morbidity and mortality is in the first hour after its occurrence, thus, being aware of the appropriate management for such factors plays a crucial role in a patient’s life [18] . Regarding Saudi Arabia, it was found that there is a lack of knowledge and practice of burn first aid in many regions [19] . Yet, there is no prior study conducted in Jazan that investigates first-aid burn perception and awareness. However, the broad objective of this study includes the evaluation of the community knowledge and attitude about BFA in Jazan City, Kingdom of Saudi Arabia with a specific target to determine the prevalence of adequate and inadequate BFA knowledge among the Jazan population. Also, find the association between BFA knowledge and different sociodemographic variables and previous BFA training. In addition, identify limitations to encourage additional research and persuade legislators to develop improved burn-injury care recommendations.
How is this paper divided?
2. Methodology
The study was designed as a cross-sectional survey using an online set of questions distributed from April 5 to May 5, 2023, in Jazan City, KSA which covers an area of 40,000 km2. And one of the most densely populated cities in the KSA. The process of data collection was done with a self-administrated set of questions hosted on the Google survey web page, and the link was sent randomly to community members in different parts of Jazan City via WhatsApp and other social media platforms. All participants were informed about the study requirements, ethically approved by the scientific research ethics committee at Jazan University. All participants who are 13 years of age and above, living in Jazan City, and those who agreed to participate were enrolled.
The sample size for this study was calculated using Cochran’s formula (n = z2pq/d2), Since there is no previous similar study in Jazan City is available, we calculated our sample size based on the assumption that 50% (P = 50%) of community population have adequate knowledge, with a 95% confidence interval and 5% margin of error. Z with a 95% CI = 1.96. P = 50% = 0.5, q = (1 − p)= 0.5, d = 0.05. → (1.96)2 (0.5) (0.5)/(0.05)2 = 384 persons.
So, the target sample size is 384. However, only 243 participants provided valid questionnaires leading to a response ratio of 63.3% considered acceptable for this study.
Data collection was done using an online pre-assessment, a structured self-administered survey consisting of 23 questions, adopted and modified from similar previous studies. The survey consisted of the following sections: Socio-demographic information: Composed of five questions about age, gender, education, occupation, and if living with children in the same house. Two additional questions were about the previous experience with burn injuries and prior burn first aid training. Knowledge: Composed of 12 multiple-response close-ended questions with the answer options as agree, disagree, do not know, such as the first correct step in first aid of burns management, covering the burn area, etc. The last section contains five questions to assess attitude.
The questions that need to be answered in this study include what are the different levels of burns first aid knowledge among community members in Jazan, and what are the associated factors that affect it? Is there a relation between prior BFA training and knowledge?
Knowledge Assessment: Each question out of 12 had only one correct answer scored as 1, while incorrect answers and “do not know” were scored as 0. A total score out of 12 was used to calculate the percentage. Scores were graded as adequate if (≥70%) and inadequate if (≤70%). Attitude Assessment: Determined as favorable or unfavorable based on responses to the five questions assessing the fire prevention and control practices and opinions. The same scoring system used in knowledge was used.
Statistical Analysis
Hejase et al. [20] contend that informed objective decisions are based on facts and numbers, real, realistic, and timely information. Furthermore, according to Hejase and Hejase [21] , “descriptive statistics deals with describing a collection of data by condensing the amounts of data into simple representative numerical quantities or plots that can provide a better understanding of the collected data” (p. 272). The data entry and analysis were performed using the IBM Statistical Product and Service Solutions software package SPSS version 26.0 [21] . Data were described using frequencies and percentages. The mean and median were calculated for the knowledge score. The chi-square test was used to find out the association of sociodemographic variables with the level of knowledge about burns prevention and first aid. All associations were considered significant at P < 0.05.
3. Results
This study included a total of 243 participants. 139 (57%) of them were in the age range of 25 - <65 years. 149 (62%) of them were males, while 93 (38%) were females. By education status, most participants 151 (62%) have a university degree and above. The baseline characteristics of patients are shown in Table 1. Regarding burn experience, nearly three quarters (72%) had a previous burn injury, and most of them were thermal (168) Figure 1. The majority of participants 75% did not take any form of BFA training in the past.
Regarding the BFA knowledge of participants, 13 knowledge-based questions were asked. The first of which was to state if a burn can lead to permanent injuries
![]()
Table 1. The base line characteristics of participants.
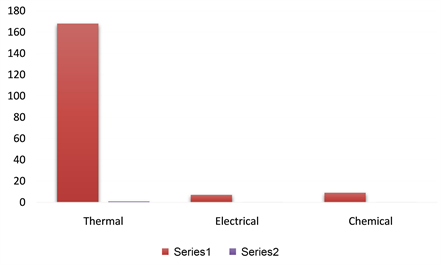
Fiqure 1. Types of previous burn injuries.
and mental disorders. 198 (82%) participants answered positively to this question. In the second question, about (106) 44% do not know the right step in case of burn injuries, which is washing the burned area with room temperature water. However, when participants were asked about the duration of washing, only 14 (8%) said they would wash for >15 minutes. Subsequently, they were asked about covering burned area with a clean cloth before heading to the hospital which can decrease the risk of infection, about (60%) answered correctly of which about 84% knew what to use to cover the burned area, denoting to clean cloth. When asked about what home traditional medication is used to apply for burn injuries, almost half of the participants (54%) answered that they would not apply anything to the burned area. 68 (28%) of responders said that toothpaste could be used. Participants’ answers to other questions are shown in Table 2.
![]()
Table 2. Participants response to Burns First Aid knowledge questions.
Then the overall mean score of participants’ knowledge was 0.60. More than two-thirds (70%) of participants were found to have inadequate knowledge about burn first aid (Figure 2).
Regarding participants’ attitudes towards BFA, four questions were asked. Only 84 (35%) agreed that applying dough, oil, mud, toothpaste, etc. on the wound delays the healing process. In addition, a significant portion (42%) think that applying traditional remedies is good for burn care before going to the health facility. The majority of the participants (98%), thought that they should learn burns first aid. Almost all participants (99%) mentioned that burn first aid is a basic skill that everyone must know. Table 3. The majority 177 (72%) of the responders, were found to have a favorable attitude toward BFA, Figure 3.
Regarding Factors associated with BFA knowledge, adequate knowledge was observed in 30.1%, of which 19% were males, and the rest 11.1% were females. A chi-square test showed no statistical significance between gender (X2 = 8.29, 9 d.f., P = 0.5), occupation, living with children at home, and previous burn injury experience. Age was significantly associated with knowledge, in contrast, old-age participants were shown to have more adequate knowledge than younger ones. Regarding education status, participants with a university degree showed more adequate knowledge. A statistically significant association was found between education and knowledge, education level and previous BFA training were statically significantly associated with knowledge level.
![]()
Figure 3. Participants attitude towards to BFA.
![]()
Table 3. Participants attitude towards burn first aid.
4. Discussion
This study focused on the evaluation of community knowledge and attitude about BFA and related factors in Jazan City, Saudi Arabia. The study observed that the majority of participants (75%) did not have any form of BFA training in the past. Additionally, the study found that 69.9% of participants had inadequate knowledge although 72% of participants had a favorable attitude toward burn first aid. Age, education status, and previous burn-related first aid training were significantly associated with participants’ knowledge of burn first aid at a P-value less than 0.05. Specifically, people with higher age and those with a university degree had a higher level of knowledge. Moreover, participants who participated in previous BFA training had more knowledge.
Similar studies have been conducted in different countries that also assessed the knowledge and attitude of communities towards BFA for example, Rostami et al. [22] from Iran found that only 4.4% of participants had adequate knowledge of burn first aid, while Khan et al. [23] from Pakistan found that the majority of participants had inadequate knowledge of BFA. These studies suggest that there is a need for community education and training in BFA to improve knowledge and attitudes towards this important topic.
Al-Mousawi et al. [24] showed that 73% of participants knew that washing with cool water was the correct first aid step for burns, which is higher than the percentage found in our study. However, similar to our study, only 7.5% of participants knew that the duration of washing should be longer than 15 minutes. Alzahrani et al. [25] in their study in Riyadh, showed that 77.7% of participants knew that washing the burned area with cool water is the correct first aid step. This study also found that only 6.3% of participants knew the correct duration of washing, which is similar to the finding in our study. Rostami et al. [22] from Iran showed that 79.6% of participants knew that cool water is the correct first aid step for burns, which is higher than the percentage found in our study. However, as with our study, only 10.4% of participants knew that the duration of washing should be longer than 15 minutes.
A study from Jordan [26] showed that 59% of the participants knew that covering the burned area with a clean cloth can help reduce the risk of infection which has similar findings with our study (60%). However, in contrast to our study which showed a higher percentage (84%) of participants knowing about covering the burned area correctly with a clean cloth as the appropriate material, the Jordanian study showed a lower percentage. Rezaei et al. [27] in Iran also reported a higher percentage (95%) of participants who correctly identified a clean cloth as the appropriate material to use for covering the burned area.
It is worth noting that although a significant percentage of participants knew about covering the burned area with a clean cloth, it is essential to emphasize the importance of using a clean cloth to prevent infection. Dutta et al. [28] in India found that the use of contaminated or dirty material to cover the burned area was associated with an increased risk of infection. A significant proportion of participants (28%) in our study believed that toothpaste could be used to treat burns is concerning, as this is a common misconception that has been previously reported in other studies. Gokdemir et al. [29] in Turkey found that 48.7% of participants believed that toothpaste could be used to treat burns. Similarly, Qadir et al. [30] from Pakistan found that 41.8% of participants believed that toothpaste was a suitable treatment for burns. These findings suggest that there is a lack of awareness among the general population about the appropriate first-aid measures for burns. It is important to educate the public about the correct first aid measures for burns, including the fact that applying toothpaste or other home remedies can be harmful and delay proper medical treatment. Healthcare professionals should take an active role in educating their patients and communities about the appropriate first-aid measures for burns. Johnson et al. [31] found that age, education status, and previous first-aid training were found to be associated with a higher knowledge of BFA. This is consistent with our study where these same factors were also found to be significantly associated with knowledge of BFA 73%.
It is promising to see that the vast majority of participants in this study recognize the importance of learning BFA. Moreover, the fact that almost all participants (99%) in our study recognized BFA as a basic skill that everyone must know, is also in line with previous research. Bilir et al. [32] in Turkey found that 99.3% of their participants believed that it is important to learn first aid skills. Similarly, Khan et al. [23] in Pakistan reported that 96.3% of their participants believed that basic first aid knowledge is essential.
Limitations
The study sample is small and represents only a fraction of the society. More extensive sudies in future can shed more light to BFA in our society.
5. Conclusion
The fact that 75% of the participants did not receive any form of BFA training in the past is a cause for concern, especially given the high incidence of burns in the region. The finding that 69.9% of the study participants have inadequate knowledge about burn first aid underscores the need for urgent action to improve education and training in this area. Despite the majority of participants (72%) having a favorable attitude towards burn first aid, this attitude alone is not enough to ensure that they can provide effective first aid in the event of a burn. The study also highlights the need to consider factors such as previous burn-related first-aid training, age, and educational status when designing interventions aimed at improving knowledge about burn first aid. Addressing this issue will require a concerted effort from healthcare professionals, policymakers, and community leaders. By developing and implementing effective education and training programs, it may be possible to reduce the incidence and severity of burns and improve the quality of care provided to burn victims in the region.