Epidemiology of Male Sexual Dysfunction (MSD) in Patients Consulting in Some Health Services in the City of Douala, Cameroon ()
1. Introduction
Sexual health is a state of physical, emotional, mental and social well-being in the area of sexuality (WHO, 2002) [1] . In both sexes, it contributes to the development of the individual through the satisfying sexual act and/or procreation. Most often, it is subject to many influences of both endogenous and exogenous origins that can disrupt the normal course of sexual activity and lead in certain situations, to sexual dysfunctions or disorders. In men, sexual disorders are grouped into four categories. These include desire disorders (translated by decreased libido and sexual aversion); sexual arousal disorders (affecting the different mechanisms involved in erection); orgasm disorders (illustrated by premature or delayed ejaculations or anejaculations) and sexual disorders with pain (which may occur during one or more phases of the act sexual (arousal: priapism; ejaculation: prostatitis) (Kaplan, 1983) [2] . Male sexual dysfunctions (MSD) can be primary or secondary, generalized or specific (to a partner, a situation...). Certain factors (age or quality of life of the patient) and/or certain pathologies (anxious-depressive disorders, cardiovascular pathologies, diabetes, dyslipidemia, etc.) can have a real impact on MSD. These factors can be either the direct cause of MSD (diabetes) or a risk or aggravating factor (age) (Rollini & Meyer, 2009) [3] . MSDs can manifest themselves at any age and in different ways during one or more phases of normal sexual activity. Depending on the severity and duration of the disease, the problems can affect the general health of the individual concerned, the balance of the couple, and even the interactions between the patient and the rest of society (family, professional level...) (El Yazidi et al., 2019) [4] . The taboo around sexual issues in our society makes it difficult to deal effectively with the acceptance of the disease to a cure. In practice, erectile and ejaculatory disorders are the most frequent reasons for consulting the doctor for sexual disorders. (Hatzimouratidis et al., 2010) [5] . Erectile dysfunction (ED) remains the most studied and medicalized pathology. His interest in research is based on its visible and symbolic character in humans (Kokel, 2011) [6] . The decision to seek help from a specialist (urologist or andrologist) is generally the consequence of several factors: loss of self-esteem, alteration of sexuality in the couple inducing an unpleasant atmosphere, incessant complaints of the partner with risk of infidelity. At the onset of a sexual problem (ED), the patient is in denial and some introversion. Given the increase in cases of MSD often translated locally by the absorption of various products and foods aimed at improving sexual performance and many prescriptions of related drugs observed in pharmacies, we asked ourselves the following questions: How to raise public awareness about the seriousness, extent and impact of sexual health problems and the need to be consulted in time? How to understand the distribution of MSD in sexually active Cameroonian people? Based on a survey, the objective of this study was to identify the different sexual dysfunctions in patients consulting in some hospitals (Deido District Hospital, Laquintinie Hospital of Douala, General Hospital of Douala) in the city of Douala, determine the associated prevalences and highlight comorbidities and other risk factors associated to these male sexual dysfunction.
2. Patients and Methods
2.1. Study Location
The study was carried out in the city of Douala, Wouri department, Littoral region-Cameroon. We worked in three hospitals of different categories in the public sector of the Ministry of Health. Category 1, a reference health facility illustrated by the Douala General Hospital, offered the highest level of care. Laquintinie Hospital and Deido District Hospital represented categories 2 and 4 respectively according to the classification of the Ministry. The choice of these health facilities guaranteed the availability of the desired specialists (urologists and/or andrologists) and a considerable sample.
2.2. Administrative Procedures
The administrative procedures were made to the officials of the University of Douala (head of laboratory and thesis director), those of the regional delegation of the Ministry of Public Health for the Littoral and the direction of hospitals concerned under presentation of the thesis project. They allowed us to obtain the research authorizations necessary for access to the various hospitals.
2.3. Reception at Study Sites
After obtaining the research certificate and the attributes of the trainee (badge) within each hospital, we were first referred to the head of the urology department (urologist) who also had the status of supervisor in a professional environment. The urologist introduced us to all his collaborators. The major of this service was responsible for responding to all concerns related to our work, including facilitating our integration into the hospital, access to certain documents (registers, patient files), and guiding us for all our needs.
2.4. Data Collection
The sample size in this study corresponded to the total number of male patients, aged at least 18 years and having consulted in the urology departments of the mentioned hospitals (DDH, LDH, DGH) between 2016 and 2020. For 18 months (Nov. 2019 - June 2021), we collected and anonymously recorded a lot of pieces of information (age, marital status, reason for consultation, health history, toxicology profile, diagnosis, profession, comorbidities, residence, assessment and treatment) contained in patient files and consultation registers available in the archives. Exceptionally, the doctor allowed us to attend the consultations to better understand the realities of the interactions between the caregiver and his patient. At the end of this investigation, the information gathered was processed and analyzed.
2.5. Statistical Analysis of Data
Data were analyzed using SPSS software version 20.0. The Mann-Whitney U test was used it possible to compare the evolution of the MSD (ED) according to age groups. A probability of less than 5% (p < 0.05) was considered significant.
3. Results
During the five-year period (2016-2020), 27446 people of both sexes and of all ages made urology consultations in the three hospitals; A total of 24,995 (91.07%) of them were male and under 18 years of age and older.
3.1. Distribution of Urology Consultations on Different Hospitals over 5 Years
Of the 24995 consultations made, 2743 patients suffered from sexual dysfunction or 10.98% of the sample. The year 2017 had the highest number of patients in urological consultation (5523) and the year 2019 had the largest of MSD cases (625). During the five-year period (2016-2020), Laquintinie Hospital had recorded the highest frequency of patients in urological consultation (13451 or 53.82%) than that (frequency) of those suffering from MSD (1770; or 64.52%) followed by the general hospital (8762; 35.05%) and finally that of Deido district (2782; 11.13%) (Table 1).
3.2. Socio-Demographic Characteristics of Patients
The average age of the 2743 MSD subjects was 44 years and the extremes were 18 and 87 years. MSD patients in the age group [31 - 40] were the most numerous (662 (24.14%)) and those aged 61 years and older were the least represented (453 (16.51%)). Marital status was divided into 1844 (67.22%) married, 871 (31.75%) single, 21 (0.77%) widowed, 4 (0.15%) divorced and 3 (0.11%) engaged. The majority of patients lived in urban areas (94.02% (2579) and lived in the informal sector at 86.99% (2174). At the occupational level, 359 (13.09%) patients were pupils and students, 301 (10.97%) were pensioners, and 86 (3.14%) were unemployed. The last professional class (1997 (72.80)) included more than 40 different trades (lawyers, police officers, drivers, carpenters, real estate agents, and painters...) (Table 2).
![]()
Table 1. Distribution of urological consultations and patients with MSD for 5 years.
DDH: Deido District Hospital; LHD: Laquintinie Hospital of Douala; DGH: Douala General Hospital; MSD: Male Sexual Dysfunction. n/year: number of patients per year
![]()
Table 2. Sociodemographic characteristics of MSD+ Patients.
MSD+: People with male sexual dysfunction.
3.3. Reasons of Consultation
Patients presented to the specialist (urologist) for different reasons (27,038 reasons) and the severity on their health concerns. The second reason for urological consultations after urinary disorders (9153; 33.85%), male sexual dysfunctions (3701) occupied an important place in urological consultations (13.69% of reasons). With the exception of urinary disorders, the reasons to be consulted by a doctor were more numerous among patients aged between 18 and 50 years. Some patients (4852; 19.95%) met the doctor for several other reasons: presentation of results, check-up, confusion of specialist, advice, scheduling of surgical interventions, non-urological pathologies (chest pain, rachialgia, digestive problems)... (Table 3).
3.4. Frequency of Sexual Dysfunction by Age and Proportion
Of the 22252 patient records browsed, 2743 were for MSD patients. Erectile dysfunction (n = 2448; 89.25%) and ejaculation disorders (n = 655; 24.12%) covering 96% of the MSD in the series, occupied the 1st and 2nd places respectively in all age groups. Patients with libido problems (n = 91; 3.3%) and painful sexual intercourse (n = 39; 1.44%) were less represented in our sample. The frequencies of EjD and PSI were decreasing between successive age groups from the youngest patients [18 - 30] to the oldest [61 and +]. In addition, it was in the 2nd [31 - 40] age group that patients with ED (n = 571) and LD (n = 34) were more numerous. More than 3 out of 4 patients and 1 in 5 patients suffered from erection and ejaculation problems, respectively (Figure 1 and Figure 2).
3.5. Prevalences of Male Sexual Dysfunction
The data collected from the various documents during our investigation allowed us to determine: the overall prevalence (10.98%), the prevalences of each form of MSD (ED; EjD; LD; PSI) and those of the different MSD according to the age
![]()
Table 3. Reasons for consultation by age.
STI/HIV: Sexually Transmitted Infections/Human Immunodeficiency Virus APIP: Abdomino - Perineo - Inguino - Pelvic.
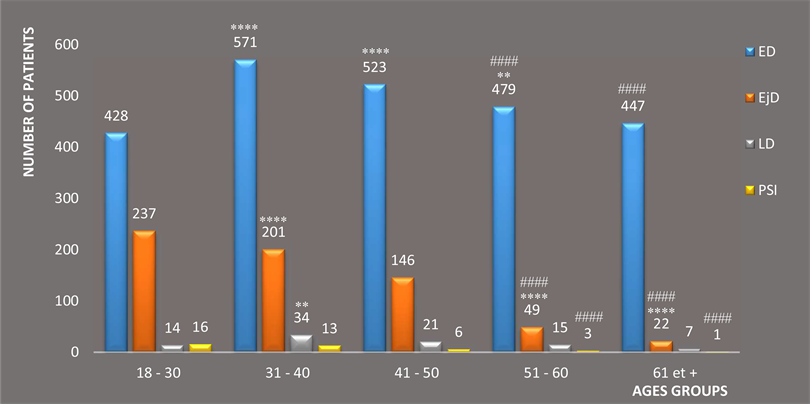
****P < 0.0001; **P< 0.01 significance of MSD between two consecutive age groups; #### P < 0.00010 significance of MSD between the youngest (18 - 30) and over 50 (groups 4 (51 - 60) and 5 (61 and +)); ED: Erectile Dysfunction LD: Libido Disorder EjD: Ejaculatory Disorder PSI: Painful Sexual Intercourse
Figure 1. Frequency of male sexual dysfunction in patients consulted by age group (n = 2743).
![]() ED: Erectile dysfunction LD: Libido disorder EjD: Ejaculatory Disorder PSI: Painful Sexual Intercourse.
ED: Erectile dysfunction LD: Libido disorder EjD: Ejaculatory Disorder PSI: Painful Sexual Intercourse.
Figure 2. Overall percentage of different male sexual dysfunctions in patients consulted (n = 2743).
groups of the study population. Erectile disorders led the way with a prevalence of 9.79%, followed by ejaculatory problems (2.62%). The last two pathologies (libido disorder and pain) had less than 1% prevalence each (Table 4).
During the quinquennium, patients in the 5th age group [61+] were the most numerous (8282 patients) and accounted for 33.13% of our study population. On the other hand, they had the lowest prevalence of MSD (ED: 5.39%; EjD: 0.26%; LD: 0.08%; PSI: 0.01%). Individuals aged 41 to 50 years were the least numerous (3233 patients) and had the highest prevalence of ED (16.17%). The highest prevalences of EjD (5.22%) and PSI (0.35%) were recorded in the youngest patients [18 - 30]. LD had the highest prevalence in patients aged between 31
![]()
Table 4. Epidemiological characteristics of male sexual dysfunctions.
ED: Erectile Dysfunction MSD+: people with male sexual dysfunctions EjD: Ejaculatory disorder MSD-: people without male sexual dysfunctions LD: Libido Disorder PSI: Painful Sexual Intercourse.
![]()
Table 5. MSD prevalence by age group.
ED: Erectile Dysfunction; LD: Libido Disorder; MSD: Male Sexual Dysfunction EjD: Ejaculatory Disorder; PSI: Painful Sexual Intercourse; n: Number of patients suffering of MSD.
and 40 years.
3.6. Pathologies and Factors Associated with Patients Suffering of MSD
Many patients had conditions and factors associated with MSD and whose distribution within the sample depended for some on age. Thus, we found an absence of hypertension, BPH and diabetes in patients aged 18 to 30 years. These cases increased gradually from the 2nd group to reach their maximum in the over 50 s. Patients with psychosocial problems and benign prostatic hyperplasia (BPH) were high among those under 50 and over 50 respectively. In the age group [31 to 40] years we found the highest frequencies of the majority of pathologies and factors associated with MSD in our sample. In general, the different comorbidities and factors associated with the MSD discussed above were distributed as follows: psychosocial problems (27%) and BPH (20%), which covered nearly 50% of this group of individuals; Testicular pathologies and cases of alcohol consumption among those under 50 years of age accounted for 13 and 15% respectively. On the other hand, metabolic syndrome diseases (diabetes (6%) and hypertension (7%) generally present in those over 50 years of age, had the lowest frequencies of factors associated with MSD (Figure 3 and Figure 4).
4. Discussion
The objective of this work was to determine the prevalences, comorbidities and the risk factors of the main sexual dysfunction in some hospitals in city of Douala.
![]() BPH: Benign Prostatic Hyperplasia; Psycho. P: Psychosocial Problems HBA: High Blood Pressure; Test. P: Testicular pathology STI/HIV: Sexually Transmitted Infections/Human Immunodeficiency Virus.
BPH: Benign Prostatic Hyperplasia; Psycho. P: Psychosocial Problems HBA: High Blood Pressure; Test. P: Testicular pathology STI/HIV: Sexually Transmitted Infections/Human Immunodeficiency Virus.
Figure 3. Pathologies and factors associated with MSD found in patients consulted by age groups (n = 2743).
![]() BPH: Benign Prostatic Hyperplasia; Psycho. P: Psychosocial Problems HBP: High Blood Pressure; Test P: Testicular Pathology STI/HIV: Sexually Transmitted Infections/Human Immunodeficiency Virus.
BPH: Benign Prostatic Hyperplasia; Psycho. P: Psychosocial Problems HBP: High Blood Pressure; Test P: Testicular Pathology STI/HIV: Sexually Transmitted Infections/Human Immunodeficiency Virus.
Figure 4. Overall percentage of MSD associated pathologies and factors found in patients consulted (n = 2743).
Through a five-year descriptive retrospective study (2016-2020), the importance of MSD in the population, their distribution according to age and some associated risk and/or aggravating factors were identified. Urinary Disorders (UD) were the primary reason for urology consultation; 1 in 3 patients complained about it and those over 50 years of age accounted for 85.79% of this dysfunction. Baka et al. [7] while working on the prevalence of ED in Morocco in 2017, highlighted the importance and a similar classification of this pathology in urological consultation. Indeed, the UD, generally put forward by the patient during a consultation, was a kind of gateway that allowed the specialist to investigate the entire urogenital system, including sexual problems. The high rate (85.79%) of patients after their fifties could be explained by the progressive enlargement of the prostate which puts pressure on the urethra by reducing its size and consequently the flow of urine during urination (diameter) (benign prostatic hyperplasia (BPH)) (Wisard and Leisinger, 2005) [8] .
The predominant sexual disorder with a prevalence of 9.79%, erectile dysfunction accounted for 76% of all MSDs in our sample. After a significant increase (p < 0.0001) of more than 33% in ED cases between the 1st [18 - 30] and the 2nd [31 - 40] age range, we found a significant decrease (p < 0.0001) in these cases between age groups 2 [31 - 40] and 3 [41 - 50] and (p < 0.01) between groups 3 [41 - 50] and 4 [51 - 60]. We also noted an 11.91% increase in ED cases between youth [18 - 30] and patients aged 51 to 60 years and 4.4% between the youngest [18 - 30] and those over 60 years of age. The frequency of ED in the 2nd age group [31 - 40] being higher, could be explained by the presence of many risk factors or aggravating ED noted in these patients such as psychological problems or depression (stress, anxiety, professional problems...), alcohol consumption, STIs/HIV and others. The involvement of these different factors and pathologies in the development and or aggravation of ED has been demonstrated by several authors. El Yazidi et al. in 2019, Wisard in 2007 and Bouhlel et al. in 2017 [4] [9] [10] showed in turn the impact of psychological state, alcohol and infections on the sexual health of DSM patients respectively. First sexual disorder in the under 30 s, Ejaculatory disorders (prevalence: 2.62%) ranked 2nd MSD (20% of MSD) of our work (after ED) were more common in the youngest [18 to 30] and were generally manifested by premature ejaculation. From the youngest patients [18 - 30] to the oldest [61 and +], between age groups 1 [18 - 30] and 2 [31 - 40], 3 [41 - 50] and 4 [51 - 60] then 4 [41 - 60] and 5 [61 and +] we found a significant decrease (p < 0.0001) in ET cases. This variation in ET frequencies was significant between the youngest [18 to 30] and those over 50 years of age and reached 91.56% between the two extreme age groups ([18 - 30] and [61 and +]). The observed result could be explained on the one hand by the irregularity and/or rarity of sexual intercourse, the lack of experience on the other hand by several psychosocial factors (stress, fear of not insuring, anxiety, trauma...) (Wisard and Audette, 2008; Gonçalves et al., 2022) [11] [12] . A similar observation on the predominance of erectile dysfunction and ejaculations was reported by Buvat et al. in 2009 [13] during their work.
Several factors identified during the study separated our population (2743 MSD patients) into two distinct patient groups: those under 51 years of age (65.48%) and those over 50 years of age (34.52%). Among those under 51 years of age, psychosocial problems ranked 1st (89.83%), followed by sexually transmitted infections/HIV (84.73%) and toxicological behaviours (alcohol use) (64.56%). For patients over 50 years of age, BPH (95.26%) was the 1st comorbidity followed by hypertension (76.31%) and diabetes (72.58%). The development, aggravation and prevalence of certain diseases in a given population are age-related. In the case of our study, many of the factors mentioned would have favoured the occurrence or worsening of a MSD and consequently its prevalence in a given population. Several authors by the choice of their sample and the relevance of their results have shown the relationship that exists between certain diseases and age on the one hand and the impact of age on prevalence on the other (Rollini and Meyer, 2009) [3] . Thus, in the case of BPH, Bagayogo et al. in 2021 [14] illustrated through their work the period of man’s life (speaking of age) to which he is most exposed to this condition (BPH). Metabolic syndrome diseases, hypertension and diabetes (such as BPH concerning age) by multiple pathogenesis (epithelial changes, endothelial dysfunction), factors such as the stage and duration of the disease, side effects of antihypertensive drugs... affect the normal mechanism of erection (Ahsaini et al., 2020; Deribew et al., 2021, Idrissa et al., 2022) [15] [16] [17] . We could not observe a gradual increase in prevalence with age for ED (predominant MSD) (9.42% [18 - 30]; 11.47% [31 - 40]; 16.17% [41 - 50]; 12.02% [51 - 60]; 5.39% [61 and +]) as revealed by some studies (Baka et al., 2017) [7] . The low prevalence (ED) among older people [61+] could be explained by the fact that sexual concerns (MSD) are becoming less and less of a health priority from this age onwards. Most often in consultation, seniors (over 60 years) favor age-related pathologies such as BPH, metabolic syndrome, low testosterone levels. These pathologies coupled with an overall decrease in sexual activity and frequency of sexual intercourse (Rollini and Meyer, 2009) [3] generally affect the quality of life of the patients concerned. The results obtained could be explained on the one hand by methodological differences (the method of data collection, the size or choice of samples) and on the other hand by the self-medication widely practised at the local level, the denial of the patient when the disease sets in and sometimes even the inability to when the disease sets in and sometimes even the inability to be consulted by a specialist due to lack of financial means. Poor retention of archives (patient records and retention records) coupled with the non-computerization of patient data within hospitals were a limiting factor for obtaining a larger sample. In addition, the lack of uniformity in the methods of consultation between different doctors and different hospitals forced us to exclude several patients so the medical data were either poorly informed or missing.
5. Conclusion
This survey allowed us to highlight the different sexual dysfunctions present in the study population, their distribution across different age groups and the risk factors (associated diseases). Although not representing the entire Cameroonian population, this work revealed some epidemiological aspects of the MSD. Thus, erectile dysfunction and ejaculation represent 3/4 and 1/5 of the MSD respectively. In addition, patients aged 31 and 40 years and those aged 18 to 30 years are the most affected by ED and EjD respectively.