Evaluation of Orthodontic Treatment Needs among Widou Schoolchildren in Ferlo (SENEGAL): A Transversal Study ()
1. Introduction
According to WHO (World Health Organisation), Malocclusion is a craniofacial or dental disorder that can lead to functional problems, with a consequent impact on face esthetics and on psychosocial aspects [1] [2] . Malocclusion became a widespread public health problem that influences life quality in a different manner [3] . Thus, comprehension of process heath-illness requires a more contextualized approach which implies questions related to health accessibility and decision of all participants to the treatment. Malocclusion has no vital risk but its impacts impose a treatment [4] . Some authors including Badran and al. [5] in Jordan, Moura and al. [6] and Thomaz and al. [7] in Brazil as well as Farias and al. [8] in Salvador studied malocclusion. Their results showed an association between sex, age, education level, social status, severity of malocclusion, dental recommendations, parent cooperation and classmate influence. Also, there is more susceptibility to others diseases and trauma added to oral disorders like mastication, deglutition and phonation. Treabart and al demonstrated their impact in life quality too [9] . In Africa, Nigeria precisely, a descriptive study investigated in 7 secondary schools, revealed that 80.3% about of students had malocclusion class I; 6.3% had malocclusion class II and 1.6% had a malocclusion class III. An open bite was reported at 7.1% of cases while crossbite was founded in 17.1% of cases [10] . In Morocco, a study on a population of 1000 children going to public schools in Casablanca, notified that 61.4% of children had a malocclusion class I; 24% class II; 10% class III and 4.6% an indeterminate molar class with one or several missing molars. More of 84% (84.2%) of children had an orthodontic treatment need. No statically significant difference has been found between sex or age and the orthodontic treatment need (p > 0.05) [11] . In Senegal, there are some data on malocclusion, particularly with Ngom and al studies but for ferlo area, this current study is the first [12] [13] [14] .
Ferlo area is an isolated locality where access is relatively difficult with almost non-existent oral care structures, oral health studies in this area are rare. People, who live there are essentially peulhs.
Peulhs are the second bigger ethnic group of Senegal and evolve in this sylvo-pastoral space, housing the Great Green Wall project (GGW) started in 2005. This project consists to value integrated development of plant and added value species. It extends from Leona to Djibouti. The Senegalese part stretches on 500 km with a wide band of 15 km. These people live with mature and develop nomadic herding as principal activity. That’s why schooling rate is very weak [15] .
The aim of this study was to evaluate the orthodontic treatment needs with schoolchildren from Ferlo.
2. Methodology
2.1. Study Type
The study was descriptive and transversal type bearing on Widou schoolchildren in Ferlo center.
2.2. Study Frame
The survey took place in Widou Thiengoly locality in the heart of space of Great Green Wall in Ferlo in Senegal center-east.
This choice was guided by geographical position of wall area, the importance of the polarized people and existence of a functional health place. This locality was characterized by their essential role in Ferlo’s the economy.
2.3. Study Population
This investigation concerned all schoolchildren living in Widou locality.
2.4. Selection Criteria
To participate to this study, children had to live in Widou or at most 6 km around the locality’s school, to be student at primary school of Widou Thiengoly; Having general health state compatible with an oral examination, having agreement of teacher and/or parents.
2.5. Sample Size and Sampling
2.5.1. Sample Size
All schoolchildren present during study were included in our sample. According to the administration, there were 126 students who were automatically enrolled in the study. In the other words, the survey was exhaustive.
2.5.2. Sampling
Given the existence of only school of Widou area and considering the exhaustive investigation, all children of all classrooms who answered to selection criteria were questioned.
2.6. Data Collect and Variables
Before the investigation started, we had sent a correspondence to medical authorities of the region for an authorization. The administration of questionary was preceded by explications on the aims and importance of people investigation for having their accord. The data were collected with WHO form establishing in 2013 and adapted to Ferlo context. The 4 investigators were students in dental surgery thesis year. They were previously calibrated and standardized for having the same comprehension, same approach and same measurement technic. This approach aimed to limit information bias. The investigation form was pre-tested on 20 people living to 50 kilometers. This allowed us to observe reaction of responding to the survey, to have estimation of times to complete the survey. The collection took place every day during april 2nd to 10th 2016 and concerned all students of Widou school who corresponded to selection criteria. The collected variables concerned socio-demographic characteristics (sex, age, schooling level), orthodontics variables (tooth alignment, aesthetic perception according aesthetic component (AC), dental health component (DHC) and need of orthodontic treatment).
For dental impression, there were used materials like impression tray with different size, alginate class A, alginate bowl, alginate spatula, gypsum, gypsum bowl, gypsum spatula, gypsum knife and hypochlorite.
2.7. Clinical Observation, Evaluation of Orthodontic Data
Variables are clinical and carried out on all students from bimaxillary impression with alginate then casted on gypsum. These gypsum models permitted to determinate the aesthetic component which consists in a scale of 10 colored pictures of teeth in frontal view, showing different levels of attractivity. The teeth aesthetic was evaluated with reference to this scale: teeth classified in 1, 2, 3 and 4 grades are considered as having no need or an insignificant treatment, those classified in 5, 6 and 7 grades are considered as having moderate treatment need and teeth classified 8, 9 and 10 grades are considered as having a proven treatment need. Dental health component records different occlusal features that characterize a malocclusion and that could contribute to morbidity of teeth and their supporting tissues. The levels treatment need are classified as following: level 5: very great need, level 4: great need, level 3: moderate need, level 2: small need, level 1: no need.
Dental health component is the result of several variables according IOTN whose teeth are missing. The absence of teeth refers essentially to 3 situations: retained teeth, agenesis and extracted teeth (Inappropriate extraction); overhang: it corresponds to distance between the edge of the maxillary incisors and the vestibular face of their mandibular homologue. These values are classified in intervals according IOTN; crossbite, is for the anterior sector when 1, 2 or 3 incisor are in linguocclusion; OIM/RC shift: is the report between mandibular position of closure characterized by the maximal intercuspidal contact and the highest condylar reference situation, realizing a bilateral condylo-disco-temporal coaptation; contact point displacement: it is measured between anatomical contact points of 2 adjacent teeth when one of them deviates from the arcade line. The contact point displacements correspond to a malposition of dental units; overbite: these are features of malocclusion which concern just incisors. supra and infraclusion are measured where they are not most pronounced. These values are classified in intervals according IOTN.
2.8. Ethnics Considerations
Before examination of each individual, his free and enlightened accord was first requested.
At the end of clinical examination, each person got a motivation and teaching of oral hygiene and received package of toothbrush and toothpaste. Information collected was confidentially treated.
2.9. Data Analysis
Data entry and analysis were carried out on the software Epi Info 7.2/Windows.
At the end of investigation 126 plugs were collected. Three of them were deleted because their gypsum models were broken or the plugs were set incompletely. Modalities of some variables were grouped in statistical calculations for epidemiological interest. We redefined and categorized the variable of age in two groups: “6 to 12 years” and “most of 12”.
So qualitative variables were grouped in proportion and quantitative variables (age) in mean and standard deviation. During bivariate analysis, we used Khi 2 of Pearson or its variant (Fisher) when there was necessary. The significance level was set at 0.05.
3. Results
With a final participation rate of 97.62% (123 students), the results obtained was as follows.
3.1. Socio-Demographical Characteristic
There was almost the same proportion of boys as girls (50.41% of girls). More of 4/5 (83.74%) of schoolchildren of Widou primary school were between 6 to 12 years old. The mean of age was 10.25 years with standard deviation of 2.15. The minimum age was 6 years and maximum 15 years. The majority (28.46%) of students in primary school of Widou were at Initiation Course class (Table 1).
3.2. Intra Dental Relationships and Static and Dynamic Inter-Arcade
Majority of sample (83.74%) presented an overjet between 0 and 3.5 mm (Picture 1). Only 1.63% of schoolchildren presented crossbite. Shift was upper to 2mm in 15.45% of schoolchildren. Contact point displacement between 2 and 4mm concerned 11.38% of schoolchildren (Picture 1).
Near 1/3 (30.08%) of sample presented a recovery between 1 - 2 mm and around 30% between 2 - 4 mm (Picture 2). Near of 1/5 (19.51%) declared that their teeth were not aligned.
3.3. Components of IOTN to Need of Proven Treatment
More of 1/10 (11.38%) of schoolchildren had aesthetic perception of classified teeth in levels 8. 9 and 10 corresponding to proven treatment needed according IOTN (Picture 3). More of 1/5 (20.33%) of schoolchildren had a score of level 4 and 3.25% of level 5 corresponding to great treatment need according IOTN.
![]()
Table 1. Repartition of sample according study level.
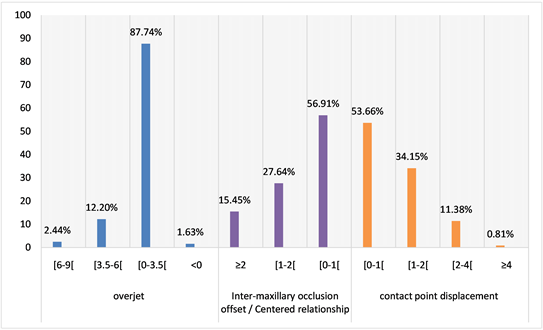
Picture 1. Repartition of sample according overjet shift OIM/RC and contact point displacement.
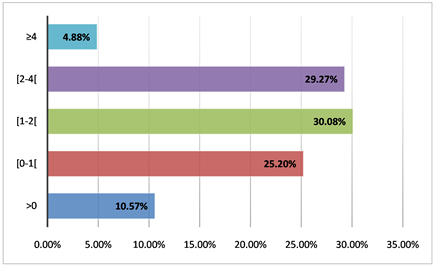
Picture 2. Repartition of sample according value of recovery.
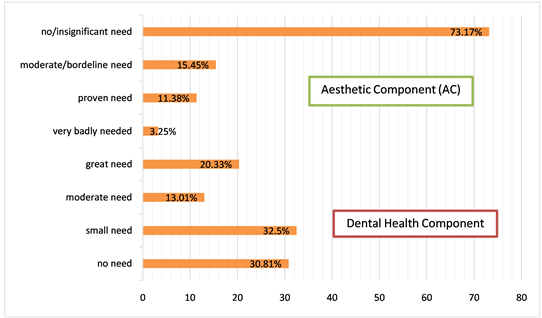
Picture 3. Repartition of sample according aesthetic component (AC) and dental heath component (DHC).
3.4. Orthodontic Treatment Need
Less than 1/4 (23.58%) had a proven orthodontic treatment need (Table 2). Proven needed treatment was more important in boys than in girls with no significant difference (p = 0.41). There is a significant statically association between the treatment needed and the age category (p = 0.013) (Table 3). Indeed, the no need of treatment was significantly lower in 6 to 12 years compared to the most of years, the moderate treatment need was significantly more important in 6 to 12 years than in more of 12 years. Finally, the proven treatment need was significantly upper in 6 to 12 years compared to the most of 12 years.
4. Discussion
Results of this work allowed to reach our goal that was evaluate the orthodontic treatment needs at Widou schoolchildren in Ferlo.
4.1. Methodologic Limit and Consideration
The study concerns part of Widou population and around which are essentially peulhs.
The peulhs are specific by their origins, culture, values and behaviors. In these specifies, it’s possible to also include, among other things orthodontic anomalies. So, it would be difficult to extrapolate the results of this study to others areas where live others peoples. However, these results could build support tools for both authorities and partners who work in Ferlo area.
For more precision of treatment need evaluation, it is usual to use x-ray like complementary examination. In Ferlo context which is rural area, it was difficult to resort to x-ray; which could underestimate the magnitude of the needs that we
![]()
Table 2. Repartition of sample according orthodontic treatment need.
![]()
Table 3. Orthodontic treatment need of study sample in function of sex, age, age category.
*Fisher test.
valued. For some variables, the asymmetry of information noted among the villagers can limit capacity or possibility to recognize or to know orthodontic existence. In the other parts, except clinical examination, a taking impressions treated with gypsum as well as calibration during the measurement carried out by only one person could allow to have valid data. This validity is all more important than study is exhaustive and takes into account all students corresponding to inclusion criteria. All these procedures of calibration, uniformization and exhaustivity help to minimize information and selection bias.
4.2. Socio-Demographic Data
In Senegal, girls represent 51.32% in preschool age, 51.9% in elementary and 52% in middle. These statistics hide the beginning of a drop in the rate of girls schooling. Besides, in secondary, the rate is 45.49% and 39.5% in university [16] . Our results showed that 50.41% of schooling people in Widou was made of girls. Then this rate stay conforms with that of the promotion of girls schooling of National Education Ministry. The study of Ngom and al. in senegalese academic place took a census of 51% of girls [13] . Besides, others studies made on schooling people through world generally had the same proportions. In London, proportion of schooling girl was 52% according to Nour Alkhatib study [17] , 51.6% in Italy [18] , 54.9% in Brazil [19] .
Our sample based on children with an average age of 12.25 years. Most of studies [13] [20] - [25] in orthodontic treatment needs according IOTN, had as population children aged of 12 years average. This age often corresponds at the start of the permanent dentition stage. That often coincides to age of orthodontic treatments. The choice of children aged 6 to 15 years is explained by necessity to study subjects both in mixed teeth than permanent teeth.
4.3. Data Which Concern Orthodontic Treatment Need
Near of 1/5 of ours ample pretended to have well aligned teeth. What differs to expression of Brazilian children who declared at 52.2% orthodontic treatment needs caused by their own aesthetic perception and their parents influence.
The low rate of aesthetic perception in Widou children is explained by their ignorance of orthodontics treatment.
Our results showed that 1.63% of students presented inverse occlusion. What bring us together of Varun results [26] 1.79%. However some authors censused a rate of occlusion inversion much more important, this is the case in Brazil [19] - [27] or in Turkey [28] but also among Indians [22] . These differences can be linked to ethnic variation. The excessive overjet located in 4 or 5 levels of IOTN and requiring orthodontic treatment, is found at 2.44% of our sample. Miguel noted this same need to 34.2% of children of Janeiro with an overjet of more than 6 mm [19] while Dias in the same state reported 12.8% of children. Other works border on results of Dias: this is the case of Nicholas [3] 11.2% to 6 years and 17.5% to 9 years; but Prassana [22] , Fundagul [28] or Varun [26] too who find respectively 11.9%, 25.1% and 17.51% of theirs subject. There is variation of overjet between boys and girls; however difference isn’t statistically significant. Among our schoolchildren widou are between 6 and 12 years, 2.91% need a proven orthodontic treatment for an excessive overjet. There are not significative differences between overage [6 - 12 years] and [12 years and more]. For Nicholas, at 6 years (11.2%) or at 9 years (17.5) the need was much more important [3] . Upper shift of 2 mm between positions in centric and maximum intercuspid occlusion was identified at brazilians schoolings [19] . The contact point displacement, manifested by diastemas or crowding represented 12.19% of our sample. This rate is relatively weak behind results of Ngom 17.9% [13] Dias 20.4% [22] or Prassana 29% [22] . The excessive overbite located in 4 or 5 levels of IOTN and requiring orthodontic treatment, is found to 15.8% of indians schoolchildren [22] ; in this same country, Singh identified rate of 13.23% [26] . These two studies, independently conducted had almost the same result. Turkey, Fundagul identified 18.3% and this rate was more represented in boys [28] . Our excessive overbite rate is weak compared with named studies above but is very over studies results [13] ruling in all Senegal country. These rates variations could be explained by ethnic diversity. Examinator perception on treatment need using aesthetic component of IOTN classed 11.38% of schoolchildren in proven need. In Senegal, Ngom and al. [13] had found at least 8.7%. This latest had comparable results to two african studies ruled by Otuyemi and al [10] and Mugonzibwa and al [29] who respectively found 7% nigerian children and 11% tanzanian children had a proven need of treatment based on aesthetic component of IOTN. At world level, our results are closer to those of Prassana 9.5% in India [22] , and especially of Andrei (11.4%) in Roumania [30] . However, values are less important in some areas: 2% in England [4] , 4.95% Sarabjeet [31] in India and 5.2% Faezeh in Iran [32] and more important in others like in Malaisya 46.7% Maen [33] or in Brazil 46.8% Miguel [19] . Evaluation of aesthetic component according IOTN, is more of purely subjective perception than an objective assessment because clinical parameters are measured in A.C. For a good treatment need evaluation with certitude, we must use D.H.C. Objective evaluation of treatment need using dental health component of IOTN had listed 23.58% of Widou students having a proven need. This proven need varies from continent to continent, country to country as it can vary within same country. These inter-country variations are underlined: in Senegal 42.6% [13] of schoolchildren aged to 12 - 13 years against 23.58% in others aged 6 - 15 years. In India we find 18.6%, 23.8%, 37.55% or 46.26% of proven need corresponding respectively to results of Prassana [22] , Faezeh [32] , Sarabjeet [31] and Varun [26] . We find in Europe values going to 15% in England [17] to 41.2% in Albania [18] . Finally, in Brazil this rate was of 34.2% [27] . If rates differ within the same age group in different populations, the cause will be linked to food behavior and ethnic variation.
Our results showed that 40% (10% + 30%) of subjects, with proven/moderate need, were more of 12 years old. What approximates the results of Ngom et al. [13] (42.6%) out of population of schoolchildren of 12 and 13 years in all the country. The age of start of orthodontic treatments starting from 12 years, the needs of Widou students show necessity of orthodontic cares. For Prassana [22] , by combining D.H.C and A.C of IOTN, reveal that 32.8% of teenagers of this sample presented a proven treatment need. Among their subjects 239 were male gender what represent 19.92% of sample.
5. Conclusion
The results of this study show that populations should be better informed about therapeutic possibilities that offered odontology in general and in particular orthodontic. Dental surgeons and other professionals of health have since then an important role in information of populations. Provision of information could proceed by formation in oral health of teachers who are in direct contact with students constituting relays to their families.