Analysis of Indigents Selection by the Community: A Construction Inequality ()
1. Introduction
Indigent selection aims to reduce health inequalities and increase the use of health services. Indigence translates into extreme poverty which constitutes a major obstacle to the use of health services in a context of pricing of acts at the point of delivery of care [1]. Several long-described methods are used to select indigents within populations [2].
In Rwanda, it is the poor at the cell level who select the poorest among themselves and then the lists are validated at the district level [3].
In some programs, indigents are identified through selected criteria and then associated with committee decisions at the village level. This method is used in Benin and Senegal but starts with community selection [4].
In other experiments, the method consists of carrying out a social survey with the help of a social worker in order to provide information based on previously defined indicators allowing the identification of an indigent person; this social survey includes interviews and home visits [5]. This method is used in Niger with the help of about ten standardized criteria Household Economy Analysis.
In Mali, in certain communes, the indigent submits a request to the commune and then a social survey is carried out in order to decide on the indigent’s situation [6].
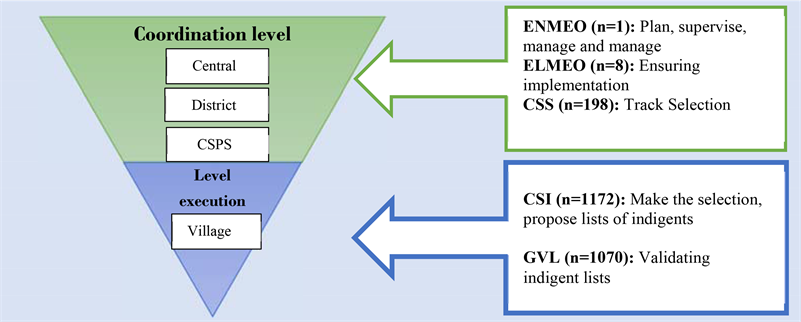
In Burkina Faso, with the support of the World Bank within the framework of Performance-Based Financing (PBF) in the health sector, it is the communities in the villages which, on the basis of a definition, selected the indigents. The selection was aimed at 15 to 20 percent indigent within the population [7]. A system composed of three coordination structures and two execution structures has been set up to implement the indigent selection process (Appendix 1). The coordination structures (ENMEO, ELMEO, CSS) are based at the central level (Ouagadougou), at the health district level and the health center level (CSPS). As for the implementation structures (CSI, GVL), they are located in the villages. A definition of destitute based on three dimensions namely poverty, disability and lack of support is used by the committee members to ensure the selection (Appendix 2).
Community selection of indigents appears to be a complex intervention and experiments show that the most effective selections have rates of 2% to 9% of indigents excluded, and less than 2% of non-indigents among indigents [8].
Although selection efficiency is commonly assessed [9], the results obtained have been the subject of few analyzes with a view to clarify decisions. In Burkina Faso, current health insurance pays particular attention to the indigent [10]. In the absence of a previous study on the quality of indigent selection in Burkina Faso, this study will contribute to filling this gap. It was made from the secondary analysis of data produced at the end of the selection. Its objective is to analyze the results and the quality of the selection carried out in Burkina Faso in eight health districts with varied contexts.
2. Method
2.1. Study Website
The data come from 4 regions of the country and concern the health districts of Ouargaye, Tenkodogo, Gourcy, Ouahigouya, Kaya, Kongoussi, Diebougou and Bâtie.
2.2. Study Design
This was a descriptive and analytical study of secondary data on the selection of indigents. The study population is made up of all the indigents selected in eight health districts of Burkina Faso following the community approach.
2.3. Data Source
The main source of information used in this study comes from the exploitation of the database of the selection of indigents carried out by the Ministry of Health of Burkina Faso between June 2014 and February 2015, then between January 2016 and December 2018 for the use of health services by the indigent. This is a database that includes all the indigents selected in the health districts concerned, i.e., 105,493 people [7].
The information used comes only from the indigent questionnaire used comprising 15 variables.
2.4. The Variables of the Study Are (Table 1)
Region, District, Commune, Village, Health center, Surname/First name, Sex, Age, Relationship with the head of household, Religion, Marital status, Level of education, Main activity, Contact details GPS, use of services [7]. The characteristics studied concerned socio-demographic characteristics, the distance separating poor households from health centres, and the use of health services. In addition, the average age and the size of the household were retained.
2.5. Statistical Analyses
The proportion of indigents selected, the proportions by socio-demographic characteristic, the average distance of selection were calculated, the number of indigents who would use health services in the years to come was estimated.
A conceptual framework composed of elements such as socio-demographic characteristics, level of selection, spatial distribution of the indigents selected, forecast of the use of health services by the indigents was used to guide the analysis.
The monthly use of health services by the indigents from 2014 to 2018 made it possible, after decomposition, to predict the future use of health services by the indigents according to the evolution of cases, seasonal variation and unexplained variation.
The time series consists of the additive model (
)and the multiplicative model (
) [11].
i: Year of observation of the series
j: Month of observation of the series
T: Trend
![]()
Table 1. Nature and modality of study variables.
S: Seasonality
E: Residues
X: Observing
In the analysis, the additive model was prioritized taking into account the amplitude of the oscillations.
The trend was estimated (
) following a seasonality of order 12 and a range of order 12.
For the calculation of the seasonal coefficient, the difference between the observations and the moving average was calculated:
. So that the average of this difference is:
N: number of years of data in the series.
This calculation will allow us to obtain first estimates of the seasonal coefficient.
The average of the first estimates of the seasonal coefficient is obtained by:
p = number of months.
The seasonal coefficient is obtained as follows:
.
The residual component corresponds to:
.
The prediction of the use of health services is obtained by Holt-Winters exponential smoothing which is a method widely used in time series predictions and is the most appropriate in short-term forecasts.
It can be modified to take seasonality into account. But this is very complicated.
Following the propositions of Holt and Winters, Tt, St and Lt can be estimated according to the following formulas:
With α, β and γ smoothing constants belonging to [0, 1];
: weighted average of the observation and the estimate of the trend at time t − 1;
: weighted average of the difference between the levels estimated at time t and t − 1;
: weighted average of the observation and the seasonality estimate at time tm. So the forecast formula is:
K corresponds to the period.
SPSS and R software were used to support these analyses. Tables and figures were prepared using Excel software.
2.6. Ethical Aspects
The study obtained the approval of the ethics committee for health research of Burkina Faso (CERS n˚ 2018-11-136) and the authorization of the health authorities of the four regions concerned: Center Est (n˚ 2019- 00191/MS/RCES/DRS), Center North (n˚ 2019-093/MS/SG/DRS-CN), North (n˚ 2019-324/MS/RNRD/DRS), South-West (n˚ 2019- 038/MS/RSUO/DRS). The anonymity of the indigents was respected.
3. Results
3.1. Sociodemographic Characteristics
Following the distribution in Table 2, the proportion of female selected indigents varied between 55 and 62% according to the districts and those of male sex from 39% to 45%. The age of heads of household varied between 20 and 98 years and over with averages of 53.2 to 61 years. The age of household members varied between 0 and 98 years with averages of 21.9 to 29.8 years.
More than 80% of the indigents selected were uneducated and less than 15% had a primary level. The secondary level was very low and higher education almost non-existent in all districts. About 60-75% of the indigents selected worked. Household members represented 50 to 65% of the composition of households against 34 to 49% of heads of household. The size of indigent households varied between 2 and 3 people.
Religiously, Muslims were dominant among the selected indigents at 51-95% in the majority of districts. The traditional religion was the most represented in the districts of Bâtie and Diebougou. The great majority of indigents were married in all the districts concerned and almost a quarter of them were widows.
3.2. Destitute Selection Level
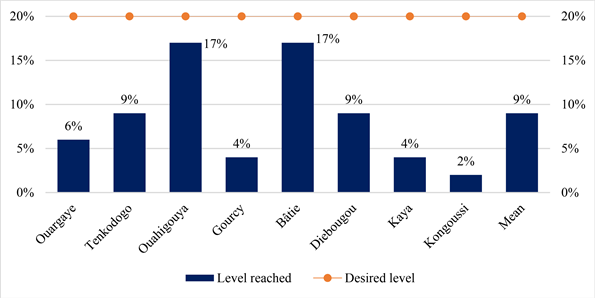
The proportion of indigents selected varied between 2% in the district of Kongoussi and 17% in the districts of Bâtie and Ouahigouya (Graph 1). The desired level of selection was 15% to 20% per health district.
3.3. Spatial Distribution of Selected Indigents
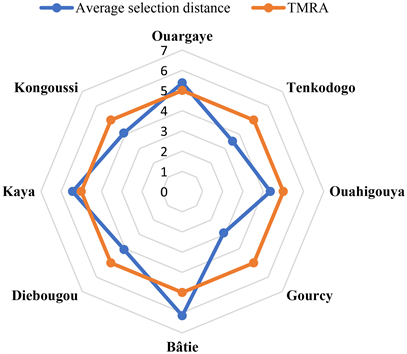
The spatial distribution of the indigents selected (Graph 2) highlights a dynamic of concentration of selection. The vast majority of the indigents selected were in households located at an average radius of 5 km from a health center corresponding to the theoretical average radius of action (RMAT) acceptable in the health system.
3.4. Forecasting the Use of Health Services by the Indigent
Compared to the level of use of health services by indigents during the period of 2014 to 2017, based on monitoring data from the Ministry of Health, forecasts
![]()
Table 2. Sociodemographic characteristics of indigents selected according to health districts.
Source: Author.
Graph 1. Proportion of indigents selected by health district.
Source: Author, based on GPS coordinates of indigent households and health centers.
Graph 2. Average distance of access to a health center by the selected indigents, and theoretical mean radius of action of the health centers.
for the period of 2018 to 2021 showed on the one hand in some districts an increase in this use of 35% in Bâtie (Graph 3), 39% in Gourcy (Graph 4), 72% in Kongoussi (Graph 5) and 20% in Tenkodogo (Graph 6); on the other hand, there was a reduction in use of services by indigents of 37% in Diebougou (Graph 7), 45% in Kaya (Graph 8), 10% in Ouahigouya (Graph 9) and 40% in Ouargaye (Graph 10).
4. Discussion
4.1. Methodological Limits
This study aimed to analyze the data collected during the selection of indigents.
![]()
Graph 3. Forecast use of services in Bâtie.
![]()
Graph 4. Forecast use of services in Gourcy.
![]()
Graph 5. Forecast use of services in Kongoussi.
![]()
Graph 6. Forecast use of services in Tenkodogo.
![]()
Graph 7. Forecast use of services in Diebougou.
![]()
Graph 8. Forecast use of services in Kaya.
![]()
Graph 9. Forecast use of services in Ouahigouya.
![]()
Graph 10. Forecast use of services in Ouargaye.
The analysis focused only on the variables entered when registering the selected indigents. The comments of the actors responsible for the selection were not taken into account in order to deepen the analyses. Also, the process used to produce these results as well as the context, in which the selection conducted was not considered.
The analysis did not take into account inclusion errors (false indigents) and exclusion errors (unselected indigents) which would make it possible to assess the quality and effectiveness of the selection.
4.2. Sociodemographic Characteristics
The female was overrepresented among the selected indigents. This means that women are more affected by poverty. This observation corroborates the results of the continuous multi-sector survey which revealed that in Burkina Faso women are more affected by poverty with an overall incidence of 52% against 48% for men, and a severity of poverty, therefore indigence, slightly higher compared to men [12]. It also emerges in Niger that three out of four poor people are female [13]. Extreme female poverty is favored by the persistent social status of “inferiority and submission to men”, especially in rural areas, they have limited access to basic social services such as education and information [14]. This result confirms the need to accentuate policies for the education of young girls and the empowerment of women.
The indigent heads of households were mainly elderly people. However, age appears to be a factor in maintaining people's physical capacities, enabling them to carry out various remunerative activities. In a context of poverty, physical incapacity compromises people’s chances of resilience and they fall into indigent. This characteristic of heads of household mirrors that noted by other studies which have shown that one of the dominant characteristics of heads of indigent households is their advanced age, at least 60 years [15]. These household heads are most often unable to work on their own, and without children to help them cultivate [16]. The influence of old age on the physical state and mobility capacities of individuals is also documented by previous research [1].
Household members were relatively younger. Being in good physical condition, young people should be able to find work to support themselves. In Burkina Faso, the population is mainly composed of young people, about 64% is under 24 years old and 77.9% is under 35 years old [12]. Globally, the poor are very young, their high proportion is concentrated in sub-Saharan Africa and nearly half of the poor were children under 15 in 2018 [17]. Interventions aimed at improving the conditions of indigents should incorporate specific actions taking into account age.
The indigents were mostly uneducated. Lack of education is one of the means that promote poverty and the deterioration of the level of health. Education is a fundamental right, an immense vector of development and each additional year of schooling increases the hourly wage by 9% [18].
Educational supply is a reflection of state policies, and demand, which is whether communities send their children to school or not, is determined by the economic resources of parents and households [19]. The low level of education of the populations is noted by other authors who found that about 82% of the population in Burkina Faso is uneducated with 89.1% in rural areas [19]. It is imperative to reinforce in a judicious and effective way the supports in the improvement of the level of education of the populations in order to increase the human capital necessary to reduce indigence.
In all the health districts concerned by the selection of indigents, many of the indigents were working. This work in fact does not constitute a buoyant and income-generating activity for the indigents which could reduce their economic vulnerability. Indeed, a survey argued that in Burkina Faso, many people work in informal activities where productivity and remuneration are low, and the general working conditions are not adequate [20]. This raises questions about employment policies in Burkina Faso, especially with regard to indigent people.
Household members were in almost similar proportions in the different districts and the overall household size of the selected indigents was small. This result differs from the situation in the country as a whole. According to the GPHC, in Burkina Faso the average size of person per household is 5.9. Several factors may explain this situation. The parents being old, they no longer have children and the older children leave the homes. Analyzes based on the standard of living approach per capita, evoke the existence of an inverse relationship between indigence and household size, other studies highlight a pre-eminence of fragile correlation through poverty indices which increase with the dimension of household size [21].
Measures aimed at following up and supporting the indigent in the fulfillment of their daily needs are necessary.
All of the indigents selected belonged to a religion and the majority were of Muslim faith. This reflects a religious commitment of the poor. This result is similar to the situation noted by the general census of the population which found that the population of Burkina Faso practiced a given religion and that six people out of ten were of the Muslim religion [22]. An analysis of the relationship between poverty and religion can increase the role of religion in improving the living conditions of the indigents.
Married indigents were much more represented in all districts followed by widows and widowers. Being in most cases adults and living in rural areas, marriage remains an important element within the community around which individual expectations and collective requirements are set and constitutes a decisive stage in the process of socialization and individual’s life. This matrimonial situation of the indigent is close to the general observation in Burkina Faso where more than three quarters of heads of household were married according to census data [22]. Accompanying measures for indigents must take their marital status into account for greater effectiveness.
4.3. The Level of Selection
Among the health districts, only two had managed to reach the desired minimum proportion of indigents to be selected. The incidence of poverty was quite high in all the districts concerned and constituted a major criterion for the application of the indigent selection. This incidence was higher than the national average (44%) and varied between 50.3% in Ouahigouya and 57.6% in Bâtie [20]. According to World Bank estimates, an expected indigence rate for the year 2015 was 9.6%. In other words, between 2013 and 2015, poverty had declined. The threshold retained for the selection then seemed not to reflect the reality of certain health districts. It is recognized that as countries move towards poverty eradication, it is increasingly difficult to be precise in estimates of the level of indigence [21]. Also, applying the same threshold to all health districts could lead to enormous difficulties or even inequalities depending on the contexts, which are very changing. It is advisable for the selection to take into account the specific context of each health district.
4.4. The Spatial Distribution of the Selected Indigents
The indigents selected were closer to health centers in the vast majority of cases. Indeed, efforts have been made in recent decades to improve the geographical accessibility of health centers in Burkina Faso. The average radius of action fell from 9.18 in 2001 to 6.4 in 2018 [23]. Other authors have noted the fact that communities have a greater tendency to select the poor who are close to health centers [24]. However, in community selection, indigent selection committees are set up in such a way as to cover all the villages regardless of the existence of health centres. Further investigations could provide a better understanding of this situation and inform the indigent select process by the community.
4.5. Forecasting the Use of Health Services by the Indigent
Forecasts for the period 2018 to 2021 showed an increase in the level of use of services by indigents in some districts, and a reduction in such use in other districts. The selection of indigents aims to improve their use of health services. The use of health services by the indigent is not only due to free care. Several other factors contribute to limiting the use of health services by the indigent [1]. This deserves to be considered in future actions aimed at improving access to health care for the indigents.
5. Conclusions
The analysis of data from the community selection of indigents conducted in eight health districts of Burkina Faso under the aegis of the Ministry of Health shows a high number of women among the indigents and heads of indigent households, mainly elderly people. Destitute households are generally small and with young people among the members. The indigents selected were practically uneducated people, practicing an activity and all belonged to a given religious denomination. Married indigents were more represented.
Also, the proportion of indigents selected varied greatly from one health district to another, both in the same region and in different regions. The minimum level of proportion to be selected was rarely reached in the districts. Indigent households were generally close to health centers.
In terms of forecasting the use of health services, the results showed both an increase and a decrease in the districts.
In a context of health insurance universal with particular emphasis on the indigent, this analysis recommends considering the level of indigents specific to each district during selection; strengthening education policies by targeting the indigents; improving the socio-sanitary conditions of the indigents, integrating specific actions considering age, gender, and marital status; formulating employment policy targeting the indigents.
Other analyzes will be able to specify the relationship between indigence and religion in order to allow the exploitation of religious capital for the benefit of the indigent to support the actions already undertaken. Also, forecasts of the use of services by the indigents will allow better planning of the care of the indigents in the current health insurance universal.
Acknowledgements
The authors wish to thank the authorities of the regions and health districts concerned and the participants for making this research possible. SIDIBE Souleymane is grateful to Prof. Drabo K. Maxime, Dr. Ilboudo Bernard, Dr. Bicaba Abel (SSRPH), and Mr. SENI Augustin.
Authors’ Contributions
All the authors participated in the study. Prof. Drabo K Maxime validated the method; Sidibe Souleymane collected and analyzed the data; all authors have amended and approved the submitted manuscript.
Abbreviations
CERS: Ethics Committee for Health Research
CN: North Center
CNRST: National Center for Scientific and Technological Research
CSS: Selection Monitoring Committee
CSI: Indigent Selection Cell
CSPS: Health and Social Promotion Center,
DRS: Regional Directorate of Health
MS: Health Ministry
ELMEO: Local Implementation Team
ENMEO: National Implementation Team
GPHC: General population and housing census
GPS Global Positioning System
GVL: Local Validation Group
PBF: performance-based financing
RCES: Central East Region
RNRD: North Region
RSUO: South West region
SG: General Secretariat
PBF: Performance-Based Financing
RMAT: Theoretical mean radius of action
SSRPH: Society for Studies and Research in Public Health.
Appendix 1. Organizational System for the Selection of Indigents and Actors
Appendix 2. Content of the Indigence Dimensions Used