Early Life Quality on Instrumental, Daily and Neuropsychological Activities of Lewy Body Disease about 70 Patients in the Geriatric Department at the Pitié Salpêtrière Hospital of Paris, France ()
1. Introduction
Lewy Body Disease (LBD) is the second most common cause of degenerative dementia. It is characterized by neuron loss and the accumulation of Lewy bodies in the brainstem, limbic and neocortical structures; in most cases, patients with LBD have the concomitant pathology of Alzheimer’s disease (AD) in the same limbic and neocortical distribution as in “pure” AD, but it is usually less extensive and can be largely limited to neurofibrillary tangles [1]. There are, however, some clinical features that are more common in Dementia Lewy Bodies (DLB) including mild parkinsonism, recurrent visual hallucinations, fluctuations in alertness [2] [3] [4]. Visuospatial and executive disorders, psychosis and apathy-depression are also frequently reported in the literature [5] [6]. The new diagnostic criteria for LBD 2017 [7] allow early evaluation of the disease through the clinic, while the 2005 criteria had underestimated the diagnostic after those of 1996 [8] [9]. The revised DLB consensus criteria now distinguish clearly between clinical features and diagnostic biomarkers, and give guidance about optimal methods to establish and interpret these. Substantial new information has been incorporated about previously reported aspects of DLB, with increased diagnostic weighting given to Rapid Eye Movement (REM) sleep behavior disorder and iodine-metaiodobenzylguanidine (MIBG) myocardial scintigraphy. The diagnostic role of other neuroimaging, electrophysiologic, and laboratory investigations is also described. Minor modifications to pathologic methods and criteria are recommended to take account of Alzheimer disease neuropathologic change, to add previously omitted Lewy-related pathology categories, and to include assessments for substantia nigra neuronal loss. Recommendations about clinical management are largely based upon expert opinion since randomized controlled trials in DLB are few. Substantial progress has been made since the previous report in the detection and recognition of DLB as a common and important clinical disorder. During that period, it has been incorporated into Diagnostic and Statistical Manual of Mental Disorders 5th edition (DSM-5), as major neurocognitive disorder with Lewy bodies [7]. It’s diifficult to tell the difference between DLB and Parkinson’s Disease Dementia (PDD). Usually, if cognitive impairment develops within a year of parkinsonism it is a Neurocognitive disorder (NCD) of LBD, while if the parkinsonism has progressed for at least a year prior to cognitive impairment it is classified as NCD of Parkinson Disease (PD). The early amyloid deposits in LBD compared to those in PD could explain the difference in the timing of dementia and parkinsonism [10]. A good quality of life lies in physical, mental and social well-being as well as the perception of one’s own health [11]. While the direct measurement of well-being through interviewing patients with neurocognitive disorders is ideal but difficult to interpret, there is also the validity of indirect measures, i.e. through the caregiver. Currently, quality of life assessments focuses largely on general dementia or AD. A systematic review regarding quality of life in dementia strongly suggests that depression is consistently linked to decreased quality life while no convincing evidence to indicate lower cognitive ability or greater activity limitations associating with a lower quality life [12]. Moreover, the measurement tools are varied, many are psychosocial for recent than objectives and practices for less recent. Our study addresses the quality of life of patients with LBD NCD to detect early IADL and NPI impairment that may interfere with quality life.
2. Materials and Methods
This is a retrospective observational study over 14 years (2005-2019) on data from the CHU Pitié Salpêtrière Geriatric Department which concerned: All patients followed or consulting a geriatrician, nurse, neuropsychologist for neurocognitive disorders with LBD (see diagnostic criteria in Table1) and having a first neuropsychological assessment at a day hospital, a completed IADL and NPI form (see TableA1 in Appendix).
The means of collection were: the data of the entered service filled in Excel, the NAS 56 server, Orbis software, the paper files in the archiving room to collect the different points of each item of the IADL and NPI scores.
We used IADL form of Lawton including the attitude or aptitude to doing 14 forms of special and daily living activities: use the phone, to go shopping, use transport, responsibility for taking medication and managing money, cleanliness, ability to eat food and dress, personal care, displacement or shift and take bath (see TableA1 in Appendix).
NB: We have by convention defined a sheet of instrumental activities of daily life IADL adapted on 11 points by concealing 3 items (Housekeeping, Food preparation, Laundry) allowing a homogeneous analysis and interpretation of the data. Indeed, it was difficult to differentiate between aptitude = possibility of carrying out an activity and attitude = objective realization of the activity. These
![]()
Table 1. Distribution of IADL by age-gender-CIRS52 of LBD patient.
activities were frequently listed as not applicable because of the presence of a third party doing it long before, but sometimes there is the problem of their attribution to gender depending on the culture.
Housekeeping, laundry and food preparation place greater demands on both executive and motor skills.
For the NPI score, we used the 12 points. Delusional ideas, hallucinations, agitation, depression, anxiety, exaltation, disinhibition, apathy, behavior Disorder, irritability sleep, appetite. The total point result of crossing the frequency and gravity of each point.
The information about IADL and NPI items were collected by caregivers interviews.
Non-inclusion criteria: other related diagnoses (vascular dementia, Alzheimer’s disease, mixed dementia, dementia of Alzheimer’s disease (AD), frontotemporal dementia (DFT), Inoperable file: IADL, NPI and YH files not fulfilled, file empty or not found. The initial hypothesis is null.
Variables study:
Global Profile of Adapted IADL and NPI in LBD TNCD
Adjustment according to age groups
Adjustments by gender
Adjustment according to the presence or absence of a motor disorder
Adjustment according to comorbidities
Adjustment according to MMS
Adjustment according to the BREF
For the statistical data, we use the Chi2 test. The hypothesis is null and the significative P value = 0.05.
3. Results
Organizational chart. LBD Patient flow and the means of variables studied.
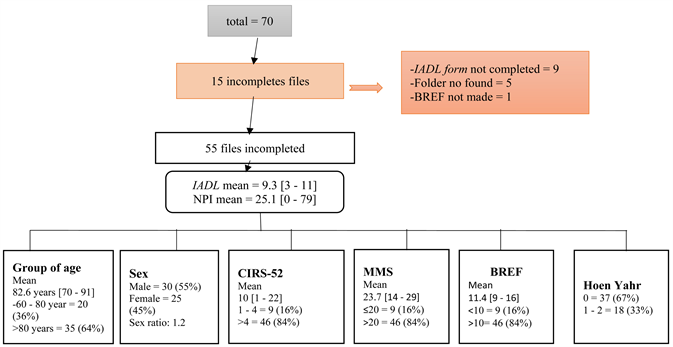
CIRS = cumulating illness rating score; MMS = mini mental status; BREF = Batterie Rapid Efficiency Frontal.
The mean age was 82.6 years old with male predominance (55%) associated of polypathology (CIRS-52 > 4 = 84%). At early stage of LBD, the major patient had moderate neurocognitive disorder according by the means to MMS, IADL, NPI scale and conserved abilities according to Hoen Yahr scale.
The LBD patient had globally conserved daily living activities specially in food, personal and bath without displacement. The most IADL activities conserved was ability to use telephone with early lost memory and race.
Ageing, polypathology were not statically changes basics and instrumental activities but was cognitive disorder statically more frequent in women (32%) than men (66%).
At early stage of LBD, as soon as MMS decrease, instrumental and basic IADL item function were alterate without disorders in abilities.
LBD patient presented globally major early humor troubles (apathy, anxiety, depression) than psychotic and behavior disorder.
NPI disorders statically increase with ageing.
When cognitive function decrease, neuropsychologic, behavior and humor disorder increase.
4. Discussion
The overall profile of early IADL impairment, regardless of the variables, affected specialized activities (64.5%) especially in medication and money management 49% and 67% respectively against for basic activities of daily life in 75.5% (Figure 1).
After adjustment aging did not appear to be a statistically significant factor influencing basic and specialized activities, regarding gender, we notice much more a disorder in the management of drugs in women (32%) than men (66%)
![]()
Figure 1. IADL global profile of LBD patient.
Figure 2. The cognitive profile of our LBD patients is characterized by a higher deficit of attentive and executive functions and a severe impairment of cognitive function in correlation of results of several studies [13] [14] [15].
Poly pathology has a statistically greater influence on functional impairment of IADL (displacement = 45%, race = 50%) than cognitive impairment of IADL (medication management = 56% and finances = 69%) by certainly causing somatic side effects. While the MMS-BREF is lower, there was more severe cognitive-motor impairment is in IADL activities (race = 22%, transport = 22%, medication management = 22%) than those of basic daily IADL (cleanliness, personal care). In studies evaluating the prevalence of autonomic symptoms in dementia, urinary symptoms, constipation, and postural dizziness were significantly higher in patients with LBD than in patients with AD [16] [17]. Using the SF-36 as a measure, higher autonomic symptom scores were linked to a lower quality of life possibly linked to limitation in basic living activities [18].
While the MMS-BREF were higher (>20), we note a dissociation between the functional impairment of IADL which is earlier (displacement = 50%, Course = 54%, transport = 56%) than the cognitive impairment of IADL (management drugs = 56% and finances = 73%) while we note a majority preservation of basic daily IADL activities (cleanliness = 78%, dressing = 80% and be personal = 86%). This trend is not classic and gives us a glimpse of the possibility of a mixed diseases association attack (Alzheimer disease and or MP Parkinson disease).
In our study, the Hoen and Yahr scale had statistically greater influence on the functional impairment of IADL (race = 22%, displacement = 27%) than cognitive IADL (medication management = 38% and financial management = 68%) in Table 2.
Consistent with our study, DLB patients from several studies had more severe functional deficits caused by motor disorders and hallucinations although the negative influence of motor disorder on ADL functional activity is known [19]
![]()
Figure 2. NPI global profile of LBD patient.
![]()
Table 2. Distribution of IADL by MMS and Hoen Yahr of LBD patient.
[20] while the correlation between specialise activities of daily living and hallucinations has not been previously reported. This result may be explained by the deficit in executive functions and by the influence of psychiatric disorders, such as hallucinations on the ability to plan activities of daily living.
The overall profile of NPI impairment is characterized by the predominance of psychological impairment (apathy = 31.8%, anxiety = 28%, depression = 25%), behavioral (irritability = 25.6%; sleep disorder = 22.9%) and psychotic disorders (hallucinations = 118% then delusions (112%) in Figure 2.
The frequency of hallucinations, listlessness and appetite was significantly higher in the LBD group than in the AD group [21].
The presence of depression and other behavioral and psychological symptoms of dementia worsens the life quality of patients with dementia and their caregivers. The presence of Lewy bodies in the limbic, para-limbic and neocortical regions may explain the appearance of depressive symptoms [22]. Early detection of depression in patients with LBD is important because these symptoms can be treated [22]. In a recently published review, the authors concluded that neuropsychiatric symptoms, particularly psychosis and depression, are priority targets for an intervention aimed at improving outcomes in patients with LBD [23]. In Ferman and al study 76% of LBD patients had a sleep disorder [24], which is characterized by nightmares, resulting in vocalizations and even violent behavior. Other nocturnal symptoms such as anxiety, periodic leg movements, urinary disturbance and difficulty rolling over in bed can contribute to sleep problems [25]. In a retrospective study of 78 patients with LBD and sleep disturbances who underwent polysomnography, 75% had experienced numerous awakenings not explained by movement or respiratory disturbance. Among the patients who did not show signs of significant respiratory disturbances, 62% of them were treated by arousals for no apparent reason [26].
After adjustment according to age, our study found a global severity of the disorders beyond 80 years and the predominance of psychological disorders (Anxiety = 346%; apathy = 325%), then behavioral (202%) and psychotic disorders (hallucinations = 165%) compared to patients under 70 - 80 years old.
The gender and poly pathology of the HY scale do not statistically influence the severity of the neuropsycho-behavioral impairment in Table 3.
In our study while the cognitive impairment (MMS-BREF) was low, there were more severe psychological disorders (anxiety-apathy) then behavioral (sleep disorder) compared to psychotic disorders (hallucinations) and even tendency when the MMS-BREF is high but with less severity compared to the low MMS-BREF in Table 4.
In the Bachard C et al. study, visual hallucinations occur in 60% - 70% of LBD patients, usually onset within the first 2 - 3 years of the disease [27]. The presentation of visual hallucinations during the first 4 years after the onset of dementia has a positive and negative predictive value for middle cognitive impairment (MCI) of 81% and 79%, respectively [28]. A recently published postmortem study [29] showed that cases of DLB exhibited reduced neuronal density in the middle gray layer of superior colliculus tissue, an important structure for directing attention to visual targets. This finding may provide pathological evidence for visual hallucinations in DLB. In a recent comparative study of 207 delusional and non-delusional patients with DLB, the authors concluded that delusional patients had poorer cognitive function and more severe neuropsychiatric symptoms [30].
Our retrospective study about early IADL and NPI impairment in LBD disease was reported by caregivers and could be not precise. Also, there are several recent tools used to evaluated life quality in chronic disease more than IADL one.
![]()
Table 3. Distribution of NPI by age-sex and comorbidities of LBD patient.
![]()
Table 4. Distribution of NPI by MMS and Hoen Yahr score of LBD patient.
![]()
Table 5. Recapitulative stage of affecting IADL and NPI functions by age, gender CIRS-52, MMS and Hoen Yahr.
+++ = severe impairment, ++ = moderate impairment, + = large impairment.
5. Conclusions
LBD has a real early impact on the quality life through cognitive, behavioral neuropsychiatric and dysautononomic domains requiring early diagnosis and multidisciplinary treatment around the geriatrician.
For early IADL impairment in the LBD was the most cognitive disorder in women; more motors disorder with polypathology; motors and cognitive disorders when MMS decrease; more motors disorders with moderate MMS and Hoen Yahr scales > 1.
About the NPI was more psychologic and behavior than psychotic one with aging and increase or decrease MMS (Table 5).
Appendix
![]()
Table A1. Revised1,2 criteria for the clinical diagnosis of probable and possible dementia with Lewy bodies (DLB).