Pragmatic Deviations in the Speech of Paranoid Schizophrenic Patients in Cameroon ()
1. Introduction
This study aimed at bringing out some Pragmatic deviations in the speech of some Paranoid Schizophrenic patients in Cameroon. The study intends to study Paranoid Schizophrenia from an African context in general and a Cameroonian point of view in particular. The study therefore seeks to report the different pragmatic lapses in the thought content and actual speech of the patients.
It is important to note that in Africa and in Cameroon in particular, people have the tendency of associating mental illness to witch craft (which is not completely false though). People are not able to trace the onset of the illness until it is too late. Some people do not even know that mental health is related to language. This study sheds light on some linguistic features that are affected due to mental illness (schizophrenia).
This study is done in the Jamot hospital, situated at the Mballa II neighbourhood in the Centre Region of Cameroon (Yaoundé). This hospital has a Psychiatric unit which receives patients nationwide, as such, the Jamot hospital is a reference centre for the treatment of patients in Cameroon.
The choice of working with schizophrenic patients was guided by the fact that most Camroonians are unaware that different types of mental illnesses exist and that there are linguistic reparcussions in the lives of individuals attained of mental disorders. Data was initially collected from patients around the streets of major cities of Cameroon, but we could not specify the particular mental illness the patients were suffering from, as such, the initial data was discarded. The actual data of this study was collected in the Jamot hospital because the hospital facility permitted us to work with psychiatrists. While taking active part in consultations and in the diagnoses processes, we were able to shortlist the different types of mental disorders that the patients were suffering from. Patients with schizophrenia presented a great degree of linguistic irregularities, which prompted us to work with them. The choice of working with mental patients is to sensitize the people on the gravity of mental health in the lives of individuals and their families.
This study therefore highlights some probable causes of schizophrenia and some therapies that can be used to help patients recover swiftly.
The instrument used in collecting data was interviewed. We used interviews because it permitted us to discuss at length with the patients and this gave us the possibility of collecting enough individual, environmental and language data for analysis. We used both quantitative and qualitative techniques in analysing data with the mathematics formula
.
Eugen Bleuler was the first to come up with the term Schizophrenia in 1911. He combined the Greek word for split, “schizo” and the Greek word for mind “phrenia”. This term was used to refer to a form of dementia, which deals with a serious thought disorder which manifests itself relatively at the early stages of life (“dementia praecox”). Research has shown that diagnoses and manifestations of schizophrenia always remain constant, despite the era and societies or communities.
It is necessary for us to mention that we will be concerned with paranoid schizophrenia.
Schizophrenia is a severe mental disorder that affects the thought, feelings and reactions of a person attained. Schizophrenics have problems distingushing between what is real and what is imaginary; they are sometimes slow or unresponsive; and they face difficulties in expressing themselves in social situations.
The causes of schizophrenia can still not be clearly determined. There are several theories on schizophrenia; some say the disease is hereditory, while others say it is biological.
Signs of schizophrenia vary from person to person. Symptoms may occur gradually over a while or may also appear abruptly. Warning signals of schizophrenia may include: hallucinations, paranoia, awful way of speaking or writing, feeling of indifference, funny body language, poor academic or work performance, poor hygiene, withdrawal, irrationality, anger etc.
Paranoid Schizophrenia is a disease that is rampant in Cameroon and the after effects are very profound on patients (Fossung, 2020).
Schizophrenia is a brain disease and it is known that language is found in the brain, so when a patient is affected by schizophrenia, it is obvious that some aspects of language will also be affected, and not only language will be affected, but the thought content, thought form and thought process will also be affected. It is also important to say that other aspects such as the psychological and social behaviour of patients will equally be impaired.
Some Cameroonians ignore the symptoms and manifestations of schizophrenia and at times they even ignore the treatment they or their patients are to follow. Doctors or psychiatrists, on their part, should not just be concerned with healing the patients, but they should think of strategies of making these patients become what they were before, especially when linguistic factors have been affected.
Linguists have a great role to play in managing mental health issues. They should be posted to work in hospitals with doctors and psychiatrists. The presence of linguists in health facilities will facilitate the detection of linguistic disorders, which may lead to prompt solutions to such problems.
2. Literature Review
2.1. Language and Thought Disorder
Schizophrenic language disorders are seen as formal thought disorders (problems are seen in thought process of patients, the content is relatively in order). McKenna et al. (1994: pp. 10-11) explain that the term comprises several abnormalities.
At times the moment-to-moment, logical sequencing of ideas could be at fault. In other instances, language production processes themselves appear to be affected. Also, the fault sometimes seems to be at the level of discourse: individual words, sentences, and sequences of thoughts make sense, but there is no discernible thread to longer verbal productions. Thought disorders can be noticed in aspects such as poor content (not expressing or providing enough information), loss of goal and other kinds of incoherence and unintelligibility.
2.2. Chaika on Linguistic Structure
The study of schizophrenic language disorder by linguists began with Cohen et al. (1974). He observed the following abnormalities:
1) Wrong use of words (failure to utter the intended lexical item);
2) Distraction by the sounds or senses of words;
3) Breakdown of syntax and/or discourse;
4) Inability to identify the abnormality of utterances.
From the above points, (2) is a good characteristic of schizophrenia. (1) and (3) are normal speech errors while (4) is a form of aphasia.
2.3. Loss of Voluntary Control
Some linguists argue that schizophrenic language disorder is fundamentally a loss of voluntary control over the speech generation process. According to Chapman (1966), patients usually express their inability to control their speech. This throws light to the main theme of the Schneiderian first-rank symptoms, which is the loss of control over the flow of thought. Lack of voluntary control often involves issues such as lexical retrieval, and sometimes pronunciation or syntax.
2.4. Andreasen’s 18-Point Scale
A good account of schizophrenic language was done by Andreasen (1979). Andreasen’s Thought, Language and Communication (TLC) scale (Andreasen & Grove, 1986) gave the basis for research and medical practice. The scale is made up of 18 symptoms and the symptoms include: “poverty of speech, poverty of content (wordy vagueness), pressure of speech (excessive speed or emphasis), distractibility (by stimuli in the environment), tangentiality (partly irrelevant replies), loss of goal, derailment (loss of goal in gradual steps), circumstantiality (numerous digressions on the way to the goal), illogicality, incoherence (word salad), neologisms (novel made-up words), word approximations (coined substitutes for existing words, such as handshoedglove), stilted speech (pompous or overly formal style), clanging, perseveration, echolalia, blocking (sudden stoppage), and self-reference (talking about oneself excessively)”. Most of the points raised by Andreasen can be reflected in the language of the patients of our study.
It should be noted that our work was greatly inspired by this 18 point scale. As we shall see, major discussions of this work are made up of some of the points highlighted above.
2.5. Communicative Behaviour in Schizophrenia
There are several concepts or theories that exist in analysing the speech of those attained of schizophrenia. The speech of schizophrenic patients is usually a cause of miscommunication and as such, it is important for their speech to be examined. It is generally accepted that features of content cause difficulty in understanding schizophrenic speech (Rosenberg & Tucker, 1979) and or form (Van Belle, 1987; Chaika, 1982; Cohen, 1978; Cohen & Camhi, 1976; Cohen, Nachmani, & Rosenberg, 1974; De Decker & Van Campe, 1989; Hoffman, Kirstein, Stopek, & Cicchetti, 1982; Rochester, Martin, & Thurstone, 1977). Meanwhile, perception is the cause of a schizophenic’s misunderstanding of his or her partner.
2.6. Schizophrenia among Sesotho Speakers in South Africa
This study was done by Mosotho, Louw and Calitz (2011) and the study aimed at investigating the clinical presentation of schizophrenia among Sesotho speakers. A total of one hundred (100) schizophrenic patients were evaluated in this study, following the Psychiatric Interview Questionnaire. The study revealed that symptoms of patients across other cultures could be found among Sesotho speakers. Cultural values greatly affect the content of psychological symptoms such as delusions and hallucinations. Symptoms such as dizziness, palpitations, headaches and excessive sweating were the most frequent among patients.
Male patients had more auditory hallucinations according to a study presented by LAUBSCHER, who carried out a study on schizophrenia and other mental disorders among Xhosa and other ethnic groups. The hallucinations of traditional patients were centered on hearing the voices of ancestors, while Christian patients heard the voice of God. Delusions of poisoning were prominent among female patients, followed by delusions of bewitchment. Delusions of grandeur among females were centered on owning cattle, land and money, and among males on having herds of cattle, many wives and much money.
3. Pragmatic Deviations
This section deals with the pragmatic features of our patients’ language.
Here we discuss the following issues: evaluation of pragmatic data, explanations and discussions. We shall also see other aspects such as pragmatic disorders, explanation of speech data, relationship between identification, speech, environmental and language data, probable causes of the disorders, consequences and therapies. We shall also analyze some pragmatic features which caught our interest and which we thought were problems that our patients were facing.
In this section, we have evaluated all the pragmatic aspects of our patients’ language and it is worth noting that we were not disappointed because we really gathered an impressive data set.
It would be good for us to elucidate here the issue of questioning. We made sure that the questions posed to the patients were clear and concise. We exercised a lot of patience and made sure that difficult questions were understood by all the patients. As such, we derived a means of asking such questions in different ways. By the way, the understanding and level of reasoning of the patients is quite outstanding, especially when they are in good shape. We made sure that we approached the patients in the mornings when they had taken breakfast and their morning medications were already settled in their systems. We also made sure to stop once we realized that they were fading away due to tiredness or stress.
We also made sure we stayed professional with them. We laughed or smiled when it was necessary and we also showed a mastery of nonverbal communication skills when we were dissatisfied with their reactions, and it is interesting to say that they understood nonverbal communication very well.
Dwelling on the pragmatic aspect of this section properly, we noticed that our patients faced a lot of difficulties with this aspect. The wide range of deviations the patients face include among others aspects such as blocking, question and answer incompatibility, incoherence, circumstantiality, pressure speech, distractible speech among others.
When the language of these patients is affected by the above mentioned deviations, it becomes very difficult to understand them as the language becomes long, winding and incomprehensible. The causes of this type of communication deficiency are explained below.
3.1. Analysis
Here, we look at the evaluation of pragmatic performances, explanations and discussions.
3.1.1. Evaluation of Pragmatic Performances
In this section we will be able to produce the various figures or percentages of the various deviations that we discovered by use of tables and diagrams.
3.1.2. Evaluation of Pragmatic Data
Table 1 below contains a synthesis of pragmatic deviations which will permit us to compare the performances of our patients and it will also help us to determine which features are more affected.
The table shows the deviation which is the most affected of this study. The figure (3) shows the highest degree of affection, (2) shows an average level of affection, (1) indicates a mild affection and (0) shows that there is no affection at all.
3.1.3. Explanations
On the basis of the data gathered, we were able to come out with this table which summarizes the different deviations suffered by our patients.
Firstly, we realized that the highest feature which affected our patients is incoherence. All our nine patients suffer from the disorder. This gives a total of 100%.
According to the table above we can notice that incoherence has the greatest number of occurrence.
![]()
Table 1. Synoptic presentation of pragmatic deviations.
SOURCE: Compiled by the author from field work, 2020.
The next features which are also highly affected are contradictory speech, pressure speech and blocking. Eight out of nine patients are involved, making a total of 88% affection rate.
Despite the fact that these three features have the same percentages, they have different levels of occurrence.
Contradictory speech occurs twelve (12) times; pressure speech occurs nine (09) times while blocking occurs eleven (11) times.
Seven (7) patients make use of incomplete speech making 77% of patients affected. Incomplete speech occurs nine (09) times.
Seven patients are affected by Question/Answer incompatibility and circumstantiality.
Question/Answer incompatibility has eleven occurrences while circumstantiality occurs fifteen times.
Furthermore, six patients (66%) are affected by distractibility and perseveration. Perseveration occurs ten times while distractibility occurs eight times.
Finally, we have phatic use of language which is the least affected feature. Three patients are affected (33%) and it has six occurrences.
These features are features which the patients use very much and they are studied here because they are issues which make the language of patients practically incomprehensible or very stressful to understand (Diagram 1).
3.2. Discussion of Results
In this section, we give a general analysis of all the pragmatic aspects of this work. We also throw some light on the analysis we have already seen above. Therefore, we will treat each deviation specifically with some examples. Note
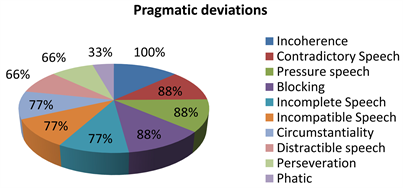
Diagram 1. Graphic representation of pragmatic performances. Source: Compiled by the author from field work, 2020.
should be taken that the examples presented cut across the discussions or utterances of our patients and no particular order was followed.
3.2.1. Incomplete Speech (Affected Patients: M1, M2, M3, M4, M6, M7 and M8)
Linguistic communication makes use of several discussion processes. Non verbal communication can lead to the interpretation of speech. Also, incomplete speech can lead someone to draw conclusions, but the meanings can only be possible when all involved share the same context. For example, the phrase “Absence makes my heart grow fonder” is well understood by all.
The speech of our patients on the other hand makes the interpretation of their language very difficult. The presence of an incomplete statement makes it rather difficult for one to know if it is an incomplete speech or blocking.
We consider this issue to be a disorder because it is recurrent and it affects more than 70% of our patients.
Generally, in the language of schizophrenics, incomplete speech can be seen at the following levels:
• At the coordination level, the patients are unable to plan their speech, which leads to the lack of appropriate ideas and words.
• At the psychological level, the patients are distracted, which prevents them from staying concentrated.
• At the dialogue level, is characterized by the inability to adjust or to improvise, leading to sudden breaks and sudden change of ideas.
Excerpt:
Examiner: What is the cause of atomic warfare?
Patient: The problem is currently …, there are two camps …
Examiner: But it’s water.
Patient: It could be water, but I don’t really …
I was rejected; in the West I have already been…, in 2007 I have already been sold.
Examiner: What do you want to invent in Physics?
Patient: Yes, what I like to do in physics is…, is…, building a nuclear power station is also… Cameroon will have to have its atomic bomb. It’s also… (pause), also establish an Aerospace research center and also… (pause), and also to build a site somewhat like the American NASA for the launching of rockets in a few years.
Examiner: Do you have a stadium?
Patient: If I have a stage it’s…
You look…, I have a word here that I don’t know…, lady. It means the charge.
Examiner: Tell me about your dating life.
Patient: If I have the people, the friends compared to… Well I thought far away or because it’s hard to understand the stories.
Examiner: And what are you still alive for?
Patient: Because eh, imagine a little… can I undress?
Examiner: Yes.
Patient: Hypertext is just a text to define of, of, of the study… Hypertext, hypertext, hypertext. Hypertext is por…, por…, por… No door, awaits protocol, angro text protocol…, angro…, angrocole.
Examiner: Do you hear or see things that others do not?
Patient: Oh those are not things that were starting, those things started in my life. They started my life until I never wanted…
Examiner: After the hospital, what will you like to do?
Patient: What I will like to do? If I never had the mind that eh, pumps so much…
Incomplete speech occurs due to several reasons. Firstly, the minds of these patients wander a lot. Once they start talking and something comes to their mind, they are unable to show priority to what they were saying before. They simply get a pause at times or try to transmit two ideas at the same time. With this type of situation, it is impossible for them to give a complete thought.
This could be seen in the examples below:
Examiner: What do you want to invent in Physics?
Patient: Yes, what I like to do in physics is… is…, building a nuclear power plant is also… Cameroon will have to have its atomic bomb. It’s also… (pause), also establish an Aerospace research center and also… (pause), and also to build a site like the American NASA for the launching of the rockets in a few years.”
Examiner: Confiscated by whom?
Patient: I don’t really know, but by people who don’t, who don’t want to see the president, His Excellency Paul Biya, evolve. So, I put down my diplomatic briefcase. That is, it is a black case containing secrets for making the atomic bomb. So what did they do? They have, that is to say all the…, at any time that I define the system they always come scrambled, scrambled, scrambled my system, scrambled, scrambled, scrambled my system so that my head is tangled. But when my head is tangled what should I do? So I have to take a little rest to sort everything out, put everything in order. In thought, in the thought sector, the reflection sector, recalls memory, memory. So that is to say, when I arrange my elements, it is always like that that we always come to lash, lash, lash. Because I remember the last day I was very angry because I had established a system to find…, regarding PMUC. A system to travel into the future and find the first five horses to be able to win the jackpot of…, how much was there? 150 million. Yeah, it was 150 million. I put all that structure together, how to make the 150 million. But and I know that to travel at the speed of light is to move very quickly and to change the notion of space-time.
Well Thursday, no we are not yet Thursday March 6th, no Thursday March 6th is coming soon. Friday, here is Friday March 7th. There will still be an opportunity to play, that is, if I want to win. How many millions is there?”
Also, the lack of knowledge about a particular subject is a cause of this deviation. When they do not master a particular topic, they tend to formulate questions which do not have answers. They are unable at times to complete what they say. For example:
Examiner: Name three objects.
Patient: Three objects?
Examiner: Three random objects.
Patient: Yes, the reunification monument on the way to the SED, well the basement, the Nlongkak underground passage, there is still e… h. Did you say to mention three monuments in Yaoundé or in Douala too?
Examiner: Three objects, not the locations.
Patient: Okay, pa.
Moreover, distraction is another cause. These patients live practically in a world of their own. They suffer from hallucinations (visual andauditory). Once they start receiving stimuli which are not evident to a normal person, they immediately respond to the commands they receive. All these distractions make it impossible for the patients to make complete sentences.
Now let us just imagine that a child asks this question: “Daddy what is linguistics?” And the father replies, “Linguistics is the study…, linguistics deals with…, the branches of linguistics are…”
I believe that if anybody were to be that child, he or she would be very frustrated. This is exactly how it is difficult dealing with the incomplete speech of these patients. It is incomprehensible and tiring and that is the reason why it is a major problem.
This nature of communication makes the language of these patients incomplete and as such communication becomes very difficult and their language very complicated to understand.
What can help these patients stop this way of communicating is by ensuring that they are not always tired and they should also take their drugs regularly. This will permit them to be more lucid and always be on ale.
They should be made to understand that the voices they hear or things they see are not real, for these things really distract them and act as a hindrance to their communication.
3.2.2. Contradictory Speech (Affected Patients: M1, M2, M3, M4, M7, M8 and M9)
Contradictory speech occurs due to the lack of concentration. A person who keeps a calm head will always be coherent even in adverse situations. Contradictory speech comes as a result of loss of memory because they tend to forget what they have said initially. The real problem is that they are not conscious of the fact that they are saying some contradictory stuff in full conversation. The two elements which are in play here are concentration and lack of consciousness.
Concentration is characteristic of a calm or cool head. It permits one to keep a good trend in conversation. A good conversation is a result of good reasoning and logic.
Excerpt:
Examiner: Are you part of a social group?
Patient: I have to tell you, the kingdom is not …, the kingdom is not …, the kingdom is me. So you have to deal with the kingdom, so the village is indeed the village, the family is indeed the family. I cannot invite the family to my kingdom. The kingdom is me. What is, you talk about family reunion, reunion is the invitation you understand. To attend a meeting you have to be invited first, but if you are not invited you cannot attend any meeting and I noticed…, as I was telling you about money power you understand a little. So you have to be someone important first to attend a meeting. According to my chaplaincy within my family already and within the social group, that means the friendly framework here.
Examiner: Do you like small children?
Patient: I like to play with big kids and I’ll tell you (laughs), there are no little kids because I like to play with … but kids get on my nerves in the long run.
Examiner: Tell me about your childhood.
Patient: It is only my mother who knows what I was like when I was born. I was a little girl, I looked like a mixed race but I was turned into a black girl. I’m there like a black American.
Examiner: You never smoked before?
Patient: No, I quit smoking.
Examiner: The bone comes out?
Patient: Yes it comes out, this place it comes out.
Your bone will come out and then the behind bone here the last place, you will stand like this without no flesh covering the bone. People will not be able to know and very soon people will not be understanding how the life is.
Loin, people have destroyed the far, this far has been destroyed but mostly women who a tying far is an abuse to them, a man who is tying far is an abuse, a Muslim who is wearing gandora is an abuse; a Muslim who is wearing white is an abuse. All those things are far; they are the people who have destroyed the loins.
They started destroying the loins since 1983 or 1982, 82 or 80, 82 so that they started destroying loins.
Examiner: Have you ever killed someone?
Patient: Yes after the person woke up, it was my older big sister. A slap from me she fell and she woke up in the evening.
From the excerpt above we can notice the following:
Eight patients are involved as far as contradictory speech or statements are concerned making a total of about 88%. Contradictory speech also occurs eight times.
The reason for this form of communication is partly because of the lack of mastery on the part of the patients. If they do not master what they are saying, they tend to come back to what they initially said.
Contradictory statements also come as a result of confusion. For example in a situation where a patient is not really sure of his age, he starts giving different figures. With this, listeners get confused and will finally not understand what they are saying because they do not give any definite answer.
Another cause of contradictory statements is lies telling. Some of these patients tell lies and at times there is no way to get the right thing from them. But there were situations in which patients gave some information but their caretakers will argue and correct them, then they eventually come back to what they said.
Anger is another aspect. There are situations in which patients are made angry by the medical staff or by security guards. When this happens, they react harshly and abuse people and in this situation they say things which they will later on regret and eventually change.
We can therefore conclude that schizophrenia hinders the concentration of patients and this makes them to produce contradictory language.
3.2.3. Question/Answer Incompatibility (Affected Patients: M1, M2, M3, M4, M5, M6, M7 and M9)
Incompability exists when there is no relation between answers that a person gives and the questions posed.
As a matter of fact, schizophrenics generally give incompatible answers to questions with total lack of interest to what is happening. From the examples below, we can see that the patients do not care about what has been asked, but they just give what comes to their mind. They express their feelings without taking into consideration what is actually bothering the interviewer.
A good sense of interpersonal communication demands that there should be satisfaction between two people who are involved in a communication process. But we can clearly see that it is not always the case with our patients, because the interviewer is not always satisfied with the responses of the patients.
In order for speech to be appropriate and complete, a speaker needs to:
• Plan and organize ideas in order to keep the trend of conversation intact;
• Gather and analyse information;
• At each occasion, integrate what has been said to ensure flexibility and to improvise for any intervention.
Schizophrenics are unable to improvise and planify, which are important production tools. This inability to planify and improvise hinders them from distinguishing certain speech acts.
Conceiving a message is a psychological activity which requires a great deal of intellectual creativity and gymnastics. Any good speaker must be able to planify before producing a good message, which is not the case with schizophrenics.
Language planning is an activity which takes seconds to carry out and people do not realize its importance at times. But it is an activity we carry out each time we talk.
Gathering and analyzing information is also an important activity. One should be able to get what others say and be able to grasp a meaning from it. It is the meaning or sense that we get from what others say that can permit us to improvise and respond properly. If we are not able to make sense from a message, then we will not be able to communicate adequately.
From the linguistic circuit of communication language planning takes place in the first phase which is conception and encoding. If one is unable to conceive ideas properly, then he or she will not be able to talk fluently and in a comprehensible manner. That person will be prone to say false things and will also have a tendency of changing things that were originally said.
Our patients are victims of this situation because they are unable to conceive ideas for a long period of time and thus are unable to give correct and cohesive answers.
Excerpt:
Examiner: Who judges people?
Patient: Directly we think that it is God to see you a little, but the one who judges, those who have judged me belong to the spiritual plane 33. So to the third spiritual plane. It was not even…, because Jesus Christ is far away on the spiritual plane 33. So that is to say it is the great masters who have judged me, the great masters who have judged me and they belong at the spiritual level only three.
Curious thing is that my file disappeared from the package, my file disappeared from the package because in the preliminary I pretended that I was the flavor of the world, that I was the messiah. Am I really that messiah there? Am I John the Baptist? Am I the messiah? Am I Jesus? Am I Jesus Christ? Jesus Christ, the One who is capable of levitation. To move he does not need… he walks in a vacuum, it is Jesus Christ there. So that is to say there are still four spiritual planes and there is John the Baptist, that is to say after 33, after the spiritual plan 33. John the Baptist who announces the coming of the messiah, then the messiah is coming, Jesus is coming, Jesus Christ is coming. So there is a difference between Jesus and Jesus Christ.
Examiner: Are there 33 plans in all?
Patient: No, there are 33 spiritual planes…, in my theory there are 33 spiritual planes in the negative sense. Where is Marie then? Where is Mary the mother of Jesus?
Examiner: How do you view Jesus?
Patient: I have a high level, I have a high level, I have a high level of thinking. I came out of the existence of lobi, that allowed me to think. So you consult with someone heavy, you consult with someone heavy.
Jesus, Jesus, Jesus, Jesus, he walked with 12 men on his return from the desert after being tempted by the serpent, he walked with 12 men. You look…, I have a word here that I don’t know…, lady. It means the charge.
Examiner: Whom did you teach? You did all of these?
Patient: Regarding all of this I grew up here. First eh I trust the wind because I was first in the village in Dschang to push, I was pushing first
Examiner: How are you feeling?
Patient: As far as my health is concerned, everything was already accomplished.
Examiner: How accomplished, how do you feel?
Patient: I had had pharmaceuticals for 21 years but it was naturopathy that saved me so that I could resume practicing the sport that I like.
Examiner: Are you married?
Patient: Marriage is the thing that is abusing. Everybody wants to abuse me about marriage. Everybody talks only about marriage, marriage, marriage. I was with my friend in Kumba; we have everything that we wanted.
Examiner: Can you hear the voices?
Patient: Now I understand that I must not run away.
There were seven patients who do not answer questions properly. Question and answer incompatibility is really a disturbing situation.
When patients are asked questions, more often than not, they give wrong answers to the questions. This really hinders the free flow of information.
Poor answers come at times due to lack of knowledge. When they do not have an answer to a question, the patients simply formulate an answer to suit the situation. It does not bother them if they are saying the right thing or not, all they are concerned with is giving a response.
Poor answers also occur due to poor timing. The patients have a lot to say, but they do not wait for the appropriate time to do so. When a patient is asked a question and he has something bothering or disturbing going on in the mind, he simply says what is going on up there in the mind and the question is of no importance to him at that particular instance.
Again, it is due to response to external stimuli. The patients do not know how to filter information or to give priority to different stimuli. It is but normal that when someone is asked a question, he/she has to react to that question, but in this context, anything which draws the attention of the patients will be given priority. It is therefore obvious that once they start reacting as such we will normally have poor responses to questions.
Furthermore, there is the deliberate refusal to answer questions properly by patients. When a sensitive topic is targeted, they seem to shy away from such topics such as incarceration, drug abuse, witchcraft etc. Due to the fact that they will not want to be disturbed concerning such topics, they will simply give answers which are not related to the topic. It is only with insistence that they will be able to say the appropriate thing.
3.2.4. Incoherence (Affected Patients: M1, M2, M3, M4, M5, M6, M7, M8, M9)
Incoherence is a situation where someone’s trend of idea is not continuous, logical nor clear. It is when one’s mind wanders from one idea to another.
A deep analysis of the language of patients permits us to discover that they are unable to produce a clear cut topic sentence. They mostly use superposed ideas which do not have any real semantic orientation. Any discourse which does not have a semantic orientation is an indication of pathology.
In order to have a coherent discussion, the speech of the theme of the listener must tie with the theme of the speaker.
A coherent discussion requires concentration and proper analysis on non verbal communication. In order to stay focused in a conversation, listeners need to know non verbal clues. They are therefore required to make use of proper eye contact, body language, stay focused, listen properly and other body gestures.
Schizophrenics do not actually make use or know these clues, which lead to discursive disorganization.
The patients rarely make use of eye contact and they also listen with a lot of distractions. This makes them to forget their trend of idea, hence they produce incoherent speech. For example:
Examiner: Tu crois en qui?
Patient: Moi, je crois en celui qui a créé l’univers, celui qui a tout créé.
Examiner: Qui a créé?
Patient: Je ne sais pas mais je crois en celui qui a tout créé. Je ne cherche pas à savoir sa vie.
Examiner: Il a un nom?
Patient: Oui, peut-être vous l’appelé Dieu, (D. I. E. U).
Examiner: Tu l’appelles comment?
Patient: Moi je l’appelle celui qui a tout créé, même la planète terre, la planète mars, la planète Venus, les étoiles dans le ciel, le cosmos.”
Concentration is highly required in order for one to follow up conversation. It permits us to retain what has been said concerning a particular theme and gives us the ability to adjust to speech. Concentration equally helps in the ordering of ideas.
Due to lack of concentration, schizophrenics are unable to put their several ideas in an orderly manner. Incoherence, therefore, is caused by poor conception of ideas and the lack of order in the transmission of these ideas. For example:
Excerpt:
Examiner: Are you part of a social group?
Patient: I have to tell you, the kingdom is not …, the kingdom is not …, the kingdom is me. So you have to deal with the kingdom, so the village is indeed the village, the family is indeed the family. I cannot invite the family to my kingdom. The kingdom is me. What is, you talk about family reunion, reunion is the invitation you kinda understand. To attend a meeting you have to be invited first, but if you are not invited you cannot attend any meeting and I noticed…, as I was telling you the monetary power you understand a little. So you have to be someone important first to attend a meeting. According to my chaplaincy within my family already and within the social group, that means the friendly framework here.
Examiner: Hello!
Patient: Hello, my name is Hilaire but it’s not Hilaire anymore. In other places I have left a birth certificate with the, with the stamp that means the gospel according to John chapter 8:1, you see nor? It means photo Fuji film for the presidency.
We’re hallelujah and now that’s what we have to do. It’s just promulgating and promoting the technological effect of churches.
Examiner: What are your secret thoughts?
Patient: I am a Christian evangelist, I am endowed with many spiritual gifts that God has given me. I was also working to build my church in my village, where my grandfather built the village catechist house on his own.
Patient: If it’s a little liquid and when I go to sleep I have to do taekwondo. So when I sleep it’s the taekwondo that comes up to look and I’m taekwondoka with the red belt. It means that I come to taekwondo, obviously life is judging me how my… What I saw at night if I see outside I score points and that taekwondity taekwondo.
I realize from the earth to go up to the sky and I love to walk and I do karate compared to this BA. I’m a ninja first. So I’m a ninja and I did my training before entering my mother’s womb, before entering my mother’s womb I finished my training.
Patient: They gave me birth in 1977, 77 I went to school in P.S Majengolo. 1980, ok 1980 since that 77 that they delivered me I was a patient of TB, TB until I reached 1980, 81, 82, 83 you see. I was in form three in P.S Majengolo. By then students were many in Majengolo and my teacher was madam X, the woman who is having a road in Mbon…, ok this is Yaoundé, Mbonge road the big tap there. Do you know the big tap?
Mbonge road, the home there was Mr. X’s home; all his children have pictured themselves abroad. Evil was following on them, you see, that was my class teacher when I was in form three. I passed to go to form three my mama said she cannot allow me to stay in this village and let me to go out and take a drug so that they should not kill me in this village.
Incoherence is the disorder which affects our patients the most. All nine patients under study made a lot of incoherent statements.
We noticed that the cause of the incoherence is due to the following reasons:
Firstly it comes as a result of disapproval. When the patients are talking and people around give a negative feedback by body language such as a shake of the head to disapprove what they are saying, it makes them to keep on talking and to say anything and anyhow. But when there is no negative feedback, their trend of idea flows logically.
Incoherence also occurs as a result of mix up of idea. It is not easy for this set of people to stick to a single idea and it is this mix up that makes them not to communicate clearly. Mix up occurs when a patient gets confused along the line and cannot terminate a thought. They tend to join almost everything that comes to their mind and say them at a blow.
This situation occurs again because of too much talking. At times when these patients start talking, they do not want to be stopped. When they start talking without stopping, they tend to talk incoherently.
3.2.5. Pressure of Speech (Affected Patients: M1, M2, M3, M4, M5, M6, M7 and M8)
Pressure speech occurs when a patient speaks rapidly as if he/she was under pressure. Pressure speech is very difficult to interrupt and hard to understand.
As mentioned earlier, concentration is key in conversation, but we should also know that calmness or a cool head is important in any discussion process. Once we are calm, we are able to control our emotions, our breath and the rate at which we speak. With calmness we are able to conceive and transmit ideas properly.
If we are able to stay calm and concentrate properly, then we are able to talk without pressure and to actually analyze our ideas before disseminating them.
This is actually not the case with schizophrenic patients. They are not capable of keeping a calm head and that makes them to lose concentration. Once concentration is gone, they are not able to control what happens to them.
The lack of concentration and pressure comes as a result of fatigue or reaction from drugs because these patients are constantly under medication.
Excerpt:
Examiner: How are you?
Patient: I am in perfect health, but it is true that I used to take the drugs that killed me, but then I understood; that is, they took four injections on the first day, hey you can send me my schedule a little there. There are references in there. That is to say, when was it already? E … h it was, it was, it was Saturday, Saturday March 1 I had two injections, Sunday two injections ok. Which already makes four injections. Between Saturday and Sunday it was four injections, which completely paralyzed me. But there is one thing chasics should know is that all movement involves a change in space of time. Well that’s the reason they’re trying to mibo…, to, to immobilize me by giving me the injections so that I sleep. Okay, so what, then what was it? Tuesday, Monday, yes Wednesday, March 5 today. On Wednesday March 5, it took…, because I no longer have a watch, but if he even had a watch… Good because I asked him if he could return to Bafoussam to bring me a mechanical watch, an electronic watch, and a magnetized, magnetized, electromagnetic watch. This could allow me now to locate the date and the day and the time. That’s what I told him, to go find me.
I think I left the instructions, I left the instructions there. I haven’t left the instructions yet because I had to write the instructions to give it. What he was supposed to collect from me in Bafoussam, which belongs to me because there is my phone. All my, most of my belongings are in Bafoussam being confiscated.
Examiner: Confiscated by who?
Patient: I don’t really know, but by people who don’t, who don’t want to see the president, His Excellency Paul Biya, evolve. So, I put down my diplomatic briefcase. That is, it is a black case containing secrets for making the atomic bomb. So what did they do? They have, that is to say all the …, at any time that I define the system they always come scrambled, scrambled, scrambled my system, scrambled, scrambled, scrambled my system so that my head is confused. But when my head is tangled what should I do? So I have to take a little rest to sort everything out, put everything in order. In thought, in the thought sector, the reflection sector, recalls memory, memory. So that is to say, when I arrange my elements, it is always like that that we always come to lash, lash, lash. Because I remember the last day I was very angry because I had established a system to find …, regarding PMUC. A system to travel into the future and find the first five horses to be able to win the jackpot of …, how much was there? 150 million. Yeah, it was 150 million. I put all that structure together, how to make the 150 million. But I know that to travel at the speed of light is to move very quickly and to change the notion of space-time.
Examiner: What does arcborge mean?
Patient: An arcborge just means new glasses that we register and that when we see, we see you moving yourself, you believe that you are a big tree but that you are also a man. It does not mean that we have a schedule that we go to put on the headphones to hear no it is wrong, it is wrong. We all work in society, don’t we? Tramp.
In the following explanation, we can notice that:
There are eight patients who are affected by this phenomenon. As we can see from the definition above, there is no apparent urgency why these patients talk rapidly and frenziedly, but from the experience and contact we had with them, we noticed that this rapid way of talking was due to a response to an external command. They will just start talking even about things which they were not asked.
Pressure speech is really a worrying situation because when they start talking it is practically impossible to stop them and when the speech is frenzied it is not easy for listeners to comprehend them.
At times these patients talk this way because according to them, they want to show others that they too can do something acceptable. So they think by talking rapidly it is going to impress people around them and give them credit.
The fact is that they feel very comfortable and rewarded when they talk this way. One thing we must note is that these patients do not reason like us and it is not really their concern if they communicate well or if people understand them or not. What they really know is that they have to communicate and any means can do. More often it is left for the listener to actually make sense from what they say.
3.2.6. Circumstantiality (Affected Patients: M1, M2, M3, M4, M6, M7 and M8)
Circumstantiality is a language condition that is complicated to comprehend because it is too long, winded and hard to reach its goal.
Just like the other features we have seen in this chapter, circumstantiality also occurs when there is lack of concentration, poor conception and distractions. The patients will be distracted and they will lose focus for a while. This makes them to give irrelevant remarks and that will lead to a delay in the delivery of the required speech. Circumstantiality is a problem because it leads to waste of time and the transmission of not very coherent ideas.
Excerpt:
Examiner: Is Paul Biya a good president?
Patient: He is a visionary, he is a visionary. His Excellency Paul Biya is a visionary because when he talks about the 2035 horizon, when I calculate, I calculate, I calculate, I calculate, I calculate, I calculate I see development, how to achieve emergence in 2035, how to reach emergence 2035. Even some people will tell you, some pessimists will tell you that it is not possible to reach emergence. Are we the date? We are in 2014, 2014 there are 21 years, 21 years left to reach emergence. What we need to do now to achieve this emergence is get down to business. If we miss our stru …, because what …, that is to say between these great …, these great presidents …; Paul Biya and so on. They are playing chess. You see a little nor.
Examiner: Tell me a bit about cults.
Patient: Well, there is a difference between there, there is a little ambiguity between the Rose-Croix and Freemasonry, not the rose-croix, but it’s all of them, they are looking for Jesus. Not to say Jesus Christ, not to say Jesus Christ because when you are already…, because I don’t know who you are. You can be John the Baptist, you can be Cameroon’s messiah, you can be Jesus, you can be Jesus Christ who comes to save us. So that is to say, these are the, I can say the grades. That is, maybe you are in such and such a rank. It all depends on how you dress, how you function, you are given the name, exactly, someone who is John the Baptist. Well, everything now depends on your way of doing, of doing, of doing, of doing, of doing, up and down, in fact. You are now given the rank of the messiah, but as long as you are not yet Jesus to reach the rank of Jesus Christ it is perfection. It really takes total perfection. There you are able to travel at the speed of light. It’s like I can throw it like that (throws paper in the air) exactly. For it to travel at the speed of light you need toh! It goes in and it appears here.
Examiner: What are you doing in the hospital?
Patient: Well I am here in the hospital because it was my mother who decided to send me here. I was discovering certain things that are not normal that parents shouldn’t do, parents shouldn’t do, parents shouldn’t do, and moms should understand. So I am having trouble with gracefully as my life went on but my life was already too stagnant.
In the three years that I have been schooling I have never written an exam, I am always sick. I’m still wondering where it comes from, what is the source of my illness. Is it a present source or a source that relates to the past? Or to continue my future did not come … Me by continuing I found solutions for remedies and my mother as a remedy I was already observed here last year in the next room there as a woman she was afraid that my illness would start again. She said no, we have to get me here to Jamot. I was brought in on a Friday and we saw Dr. Kamga who was my psychiatric doctor with whom I chatted for a long time, but now I got here, I took the injections, I took the injections. The last injection I took I took this Thursday night.
You see it kinda makes me a little weird to understand that a mother who does not know how to put a child in stability, you see a little bit nor, and a volatile father. It comes when you are there or when you are not there, like a blinker, it is not normal.
Examiner: Did you hear the voices?
Patient: At that time I could not yet hear the voices that speak to me now, as they speak to me a lot now. Imagine getting ready to go get five hours of sleep, poh! Directly at three o’clock I am told that get up, do such and such a thing, do such a thing, do such a thing, do such a thing, do such a thing, do such a thing. I understood that it is the great masters who are talking to me. The great masters of Franmasonnerie, of the Rose Croix, the grand masters of …, the leaders, the leaders of the churches.
Examiner: How often are you restless or tensed?
Patient: That’s not …, life, life has already done me tricks on a level where people only find me in tension you see a little, that when someone only comes and he finds it tense. Since you arrived here today, I have a little time to think about it. Okay as you came here, the next person who is going to tell me something I will no longer be happy. Okay today you say hello to me, I said what is it? It’s after I have thought about it that I say but why did I answer him like that, I have no problem with, that’s why I came to talk to you.
From the examples above, we can notice that the patients do not go directly to the point when they are required to talk. They beat around the bush and say irrelevant things.
The speech they produce is winded and convoluted. All these long speeches make their language and discussion incomprehensible.
This situation occurs when these patients are not ready to talk. Yes they are talking, but they do not really want to tackle the topic or problem they are faced with. They tend to talk about things of their past which is not related to the topic at stake.
What we can notice is that they have the tendency to talk about their past, witchcraft or politics. Once a question touches the pain that they feel, instead of answering the question directly, they will start explaining other things before actually getting to the point of focus.
3.2.7. Distractible Speech (Affected Patients: M1, M3, M4)
Distractible speech occurs when one changes the subject under discussion because of external stimulus.
Distractible speech generally occurs due to the influence of external stimuli. Speakers should be able to discriminate and choose the right stimulus to react to. In our everyday lives we are distracted by several things happening around us. For example, a student attending lectures should be able to choose the right option from the following external stimuli; counting cars passing by the road side, listening to music played by a publicity van or listening to the voice of the teacher. A greater percentage of students will choose listening to the teacher’s lectures. On the other hand, schizophrenics will tend to fall for external stimuli.
Excerpt:
Examiner: Do you think the devil exists?
Patient: But how not to. All these people there, whether it be the devil, Satan, Lucifer, they exist. You can’t know who is who… (Talks to brother: why are you looking at me?)
Examiner: I’m talking about your village.
Patient: My village, I am a girl from the center. My native village is Jamot, my native village is Jamot and my center (talks to a passerby) hello madam, you know me well nor?
Examiner: Was that your mind that went there?
Patient: With my whole body.
(Distracted) My brother do you want to be consulted by Dr. Kamga? Here is his counterpart.
Examiner: How many times?
Patient: When my first baby was 11 months old I had this mental illness because I wanted to do a what? I had made a cornfield with my first husband. The mango is not yet ripe.
Do you understand this bird? He says it rains fast Jacky, it wants me to wash up.
Examiner: And what are you still alive for?
Patient: Because eh, imagine a little… can I undress?
Analysis shows that only three patients are affected by distracting speech. This phenomenon occurs simply because the patients are influenced and distracted by external stimulus. When they get distracted, they stop what they were saying and they will not come back to what they were saying. This is a problem because they will be unable to complete their thought.
3.2.8. Perseveration (Patients Affected: M1, M2, M4, M6, M7, M9)
Perseveration involves persistent repetition of words or ideas.
With a well-conceived idea, people are able to communicate in a free and fluent way. The use of imagination and creativity leads to a higher level of interaction among speakers. When we also organize our speech, we are able to transmit it well. Proper organization and conception permit us to readily have words and ideas to communicate.
Patients suffering from schizophrenia are unable to think, organize and communicate properly. They tend to run short of words and ideas. In order to compensate for that, they repeat words and sentences over and over. These repetitions do not have semantic meaning and thus make comprehension very difficult.
Excerpt:
Examiner: After the hospital, are you going to continue with the work of the kingdom?
Patient: Yes, I also succeeded in being a crossroad, a colored crossroad, I succeeded in being a crossroad, I succeeded in being a crossroad.
Examiner: What is hypertext?
Patient: Hypertext is just a text to define of, of, of the study … Hypertext, hypertext, hypertext.
Examiner: Do you have the degree?
Patient: Okay, if you want me to enter a bachelor’s degree, but I prefer the sciences of mathematics, but since I trained in French-speaking law, I am not in English law. I did French law and Anglophone law eh… Kizanie, kizanie, kizanie, kizanie, kizanie of the faculty, kizanie, kizanie, kizanie of friendship. I did French-speaking law through the ten commandments of Moses, love your neighbours as yourself. I learned law.
Examiner: Your sister told me you were given 5000 FRS, what did you do with the money?
Patient: I went with the 5000. I said this money I have to sacrifice this money for this room, this room that they have being tormenting me all through. See because since I came to this room excreta, excreta, excreta 5 times, excreta 6 times in the night, not the posh but fat excreta.
Examiner: What is a World War?
Patient: Yes a world war and it will be catastrophic. They must prepare; get ready, you get ready, you get ready. In three, in three, in three, war, in three, in three, in three, in three, three, three, three, three, three, three …
Examiner: What time is it?
Patient: Wait a minute and see; well on time when I took the last hour of this Wednesday, March 5, it was 9.35 a.m., 9.35 a.m., 9.35 a.m., 9.35 a.m., 9.35 a.m., 9.35 a.m., 9.35 a.m. What time is it over there at your place?
Examine: What is the analogue system?
Patient: Ah, the analogue system, we’ve been there since. Currently we are still trying to get to the digital system. In other words, the binary system where we respond with true or false, true or false, true or false, true or false, true or false, true or false, true or false, true or false. False, True, False, True, False, True, False, True. True, true, true, true, true, true.
Examiner: How do you view Jesus?
Patient: Jesus, Jesus, Jesus, Jesus, he walked with 12 men on his return from the desert after being tempted by the serpent, he walked with 12 men. You look…, I have a word here that I don’t know…, lady. It means the charge.
So the degree of the church, the church must also learn to listen, listen to the discoveries because I had a problem with give your life to Jesus, give your life to Jesus, give your life to Jesus, give your life to Jesus, give your life to Jesus, give your life to Jesus.
Examiner: Tell me about social or political facts.
Patient: Politics yes because politics, because politics, politics, politics allow free expression.
Examiner: How many children would you like to have?
Patient: Three, three, three, three, three, three princes. So three children, five, five, five.
Examiner: Are you working?
Patient: Prayer, I went to pray and my money is coming out of there, so it’s a job. Prayer, when I pray he listens isn’t it? Yes that means that it must do a job. I have protected my country a lot from childhood to college, protection for 100,000 years. For 7 days, 7 days, 7 days, 7 days, 7 days I prayed for seven days.
Very soon this bone will come out, very soon this bone like this will come out, very soon this bone like this will be out.
Examiner: What do the voices you hear tell you?
Patient: Ah the voice I hear, I haven’t heard the voice these days. I haven’t heard the voice these days. I have not been hearing it.
Six among our nine surveyed patients suffer from perseveration. As can be seen from the examples above, the patients have the tendency of repeating words, phrases and sentences. There is no apparent stimulus which pushes them to do so, but we think perseveration is their own way of making themselves heard. With repetition, people will get to notice them or what they are doing and will therefore pay attention to them.
With perseveration they really hardly communicate any clear idea. They keep on saying one and the same thing which actually brings no particular contribution in the discussion process.
3.3. Pragmatic Disorders: Relationship between Psychiatric, Cognitive and Psychological Hypotheses
The reason why we look at the relationship between psychiatry, cognition and psychology is simply because we want to understand how the minds of patients function vis-a-vis language.
By creating a relationship between linguistics disorders and psychology, we can easily say that schizophrenic patients have lost the usage of their right hemisphere. It is important to remind ourselves here that the right hemisphere is in charge of thought, semantics, pragmatics and prosodic elements. Thought can only be manifested through the language we use. In the speech of our patients we could easily perceive that they had cognitive and psychological problems. This could account for the reason why they usually gave wrong answers to questions; and why they went out of topic at times. Patients also could not conceive ideas properly and this was a major hindrance to their language and communication.
In order for language to be transmitted coherently and without any pragmatic difficulties, speakers must be able to conceive and plan, and this task takes place in the right hemisphere. Note should be taken that schizophrenics do not lose the proper use of language, but they lose the proper usage of their thought. Language can only come through thought and thought can only be manifested through speech (language). If by some reason we are unable to think straight and conceive clear ideas, we are prone to talk anyhow and to make a lot of mistakes. Poor thought and conception may lead to confusion, repetition, blocking, neologisms, perseveration, incomplete speech among others. This could be illustrated with the examples below:
“Patient: Hypertext is just a text to define of, of, of the study … Hypertext, hypertext, hypertext. Hypertext is por…, por…, por… No door, awaits protocol, angro text protocol…, angro…, angrocole.
Examiner: What level of education do you have, what degree?
Patient: The diploma I have very …, because I am already at CRTV. You even in your system I can know you because you go off the radio maybe and I was even there in the presidency and it is there that the dictator himself is waiting, the BIR himself.
Examiner: What is the greatest level in taekwondo?
Patient: It depends on the grand master. The great master for me is God, the great master for me is God who has been…, it is God”.
We can say here that the left hemisphere of schizophrenic patients is quite intact. From the language of the patients we can see that the basic language elements such as phonology, morphology and syntax are used properly.
The relationship between coherence and cognition shows that the incoherence seen in schizophrenic patients is as a result of their inability to coordinate and maintain discussion with others. This inability to coordinate properly leads to poor control and transmission of intensions. This makes us to conclude that schizophrenics do not react consciously but they react in an instinctive, unintentional and unconscious manner. This can easily explain why schizophrenic patients are at times timid, aggressive, agitated and reserved. There are times that the patients did not want to talk or even see anyone. At times they are put in chains and isolated so as to avoid any unpleasant situation. Some examples are shown below:
“Examiner: Tell me a little bit about yourself?”
Patient: What I like. I don’t like to be disturbed, I like to be alone, I like music, I like movies, I smoke cigarettes, I also smoke joint.
Examiner: Would you like to have people with you?
Patient: People, people are my family, my family and my friends. At my age I couldn’t make any real friends, you kinda understand.
Examiner: Will you accept if I want to marry you?
Patient: Yes.
Examiner: Why?
Patient: Because you are smart like me.
Examiner: Is that all?
Patient: Yes, man is first of all intelligence with courage. You had the courage to speak to me because I am very mean. Wickedness towards what? Because the man who gives birth to the children always abandons the children there. He lets me suffer with the grandmother. You, you are a journalist, I am a journalist from the radio. All the waves are listening to us now. Did you see, whose bump is that? The hump of the man.
Examine: How are you today?
Patient: Good eh…, good eh…, good eh… I’m fine. What is the problem that brings you against me?
Examiner: I have no problem.
Patient: Okay what’s the problem …, good …, good because …, it’s because it’s already Monday nor. Today whatever security guard touches me I will beat him to death today. When I say death it’s because when I strike with all the strength inside me I can kill you.
Moreover, pragmatic disorders occur as a result of patients not being able to perform cognitive acts properly.
Schizophrenic patients suffer from hallucinations and delirium. These psychiatric disorders lead to pragmatic deviations. The appearance of these symptoms leads to the inability to transmit proper intentions to others. Patients hear things that others do not hear and this makes them to say things which are at times out of place.
All in all, schizophrenics cannot properly make use of the very first phase of the linguistic circuit of communication which is conception.
We should always be able to make a link between what is said verbally and what is non-verbal.
3.4. Explanation of Speech Data
Non-verbal communication deals with the sending of wordless messages. It involves the use of body language. Sometimes nonverbal responses contradict verbal communication which usually affects the effectiveness of the message.
Non-verbal communication deals with following features:
1) Appearance
Appearance generally deals with personal hygiene (clothing, hairstyle, neatness, use of cosmetics) and the surrounding or environment (room size, lighting, decoration, furnishing etc.). The appearance of our patients revealed a lot from first sight. It was common to find wounds all over their bodies. This was as a result of struggles that they had with security men who had to use force to restrain them. These patients were really uncombed; with flies around them and strong body odor. They were always isolated and proved to be very aggressive towards strangers and visitors at times.
2) Body Language
Facial expressions, gestures, postures.
According to our speech data, we realized that our patients avoided eye contact. They rarely smiled or laughed nor even frowned. This made it difficult to interpret their emotions. There were times that some were very aggressive especially at the initial stage when we tried to initiate contact with them. There were periods that they were very silent and refused to say anything to anyone.
3) Sounds
Voice Tone, Volume, Speech rate
As we illustrated with circumstantiality and other pragmatic features, there were periods that the surveyed patients talked frenziedly and very rapidly. At times their tone was very high that it seemed they were shouting and in other situations their tone was too low that we had to urge them to talk louder or pay more attention to what they were saying.
From the notes above, we can clearly see that nonverbal communication is as important as verbal communication. If we can master the techniques and clues of nonverbal communication, then we will become great communicators.
As we have seen the three elements of nonverbal communication above which are appearance, body language and voice, we can say that schizophrenic patients fall short of these elements. The patients do not dress properly and their personal sanitation is a call for concern. It is very common to find these patients with wounds and flies turning around them.
The patients do not know how to use body language. The first element we will discuss under body language is the use of eye contact. Proper use of eye contact will permit one to interpret a message well or not. It is normal to focus your eyes on a speaker during discussion, but the look should not be exaggerated. But the case with most of our patients is that they rarely make eye contact.
Another aspect is facial expression such as smiling or laughing. The patients do not know at all when they have to smile or laugh. It is not proper that when someone is being asked a question and instead of concentrating and answering the question, the patient starts laughing or smiling. There are times that these patients just smile for no good reason. It is abnormal for a person to smile for more than ten minutes, but these patients can go for up to an hour just smiling. This makes it difficult to actually interpret their nonverbal language.
The other aspect which we would love to talk about is the voice of patients (amplitude). They do not know how to control their tone, volume and speech rate. There are times that they speak very loud, which make it difficult for people to get what they say. At other times, they talk so low that not a single sound can be heard. As far as speech rate is concerned, we have seen that patients talk frenziedly and with a lot of pressure which makes it difficult for their speech to be interpreted. Our speech data also shows that 88% of patients use a lot of threat. Once they are contradicted, they either express threat verbally or they express anger facially.
Seventy-eight of the surveyed patients are aggressive, especially when they meet people for the very first time. Their illness is the cause of this aggressiveness because they are not in total control of their emotions.
Interestingly, 100% of patients soliloquize. They have the tendency of speaking to themselves or in solitude. This situation occurs at times because of hallucinations. They see and hear things which other people do not see.
Apart from the negative aspects we have discussed above, schizophrenic patients manifest some positive behaviour such as respect of people, they are able to play, they cooperate, they are able to recognize people and they are periodically friendly.
3.5. Relation between Identification, Speech, Environmental and Language Data
In this section we will look into the causes, consequences and therapeutic approach followed by schizophrenic patients.
From identification data we can realize that 78% of our patients (7 out of 9) are males while 22% (2 out of 9) are females. From our study therefore, we can see that women are less affected than men.
Schizophrenia is an illness which can affect people of all classes and levels of education. From our identification data we can see that 78% of patients have at least an Ordinary level certificate. So we can confidently infer that illiteracy is not the cause of schizophrenia.
3.6. Probable Causes
Our environmental data permits us to draw the following conclusions:
• 100% of patients are still bachelors and none of them is independent. It becomes very stressful and frustrating at a certain age when someone is not yet married. Socially it becomes a problem when people are not married especially from an African perspective.
It is not only a social problem, but it becomes a family problem too. African parents will expect that as from the age of 25 or at most 30 a son or daughter should be able to bear at least a grandchild.
Another issue which people have to handle is the economic factor. Unemployment rate in Cameroon is alarming. How then will young people be able to get married if they do not have jobs or are not financially viable? This too makes the patients to undergo a lot of difficulties. It is worth noting that none of our patients was employed. All these social and economic aspects can cause mental instability.
• 67% of patients used drugs or consumed alcohol. Alcoholism or drug abuse is very common in the Cameroonian society today. Most young people who go to hospital have either taken drugs or abused the intake of alcohol. Alcohol or drug abuse has negative effects on the cerebral cortex. Apart from people suffering from mental disorders, it is common to find young people who suffer from temporal madness due to the consumption of alcohol. It is common to find people get out of control once they have taken excess alcohol.
We can therefore say that alcohol or drug abuse can lead to mental disorder.
• 22% of patients M1 and M5 have a history of people who have suffered from a mental disorder. This goes to tell us that schizophrenia is not hereditary.
• 78% of patients believe in witchcraft. They all say that their illness was inflicted on them by either their parents or some aunty or grandparent. We cannot refute the fact that witchcraft exists in Africa and it is a possibility that these patients have been made sick by someone, but this theory still needs to be taken with a grain of salt.
• 78% of patients have followed other treatments apart from going to the Jamot hospital. They followed treatments with traditional healers. The reason why they went to traditional healers was due to the fact that they believed their illness was as a result of witchcraft. But after some months or even years and with no improvement, they decided to visit a specialist in a specialized hospital. And as a matter of fact, since they went to hospital their conditions have significantly improved.
• All patients interact with people. This tells us that schizophrenia does not totally affect the social abilities of patients.
• None of our patients suffered from any congenital illness. Which means schizophrenia is not acquired from birth, but due some social, psychological and economic factors.
3.7. Consequences
Schizophrenia is a disease which has negative effects in practically all aspects of a patient’s life.
The illness can have effects at the following levels: social, individual, economic and even on the nation.
At the individual level we can find the following effects:
The illness has a negative effect on the future of the patients. With schizophrenia, the life of patients literally comes to an end. They are not able to set goals; they have no purpose or focus in life. The life of a schizophrenic is practically controlled by others. With the loss of the sense of reality, patients need their families by them to help them do even the most basic of things like personal hygiene and eating.
They spend most of their time in hospitals. People will also have to tell them what to do. They are not capable of taking decisions on their own.
These patients become a liability to their family members. As a matter of fact, the life of schizophrenic patients centers on drugs and medications.
The worrying issue is that in Cameroon there is no adequate health insurance policy. All the charges of these patients are borne by their already poor families.
With this illness, patients tend to lose their jobs because they are not required to carry out difficult intellectual activities.
At the family level, the following effects can be felt:
From an economic perspective, mental illnesses are very difficult to treat. The drugs are very expensive and the follow up is tedious.
Parents or family members have to make enormous financial sacrifices to assist these patients. They spend a fortune at the level of the medical tests that they have to carry out, at the level of consultations and also at the level of hospitalizations. It is important to mention that hospitalization is very expensive.
The illness also requires the sacrifice of time. Family members have to reorganize their schedule to meet up with those of the patients. Patients have fixed time that they need to take their drugs, and as such, the family has to be able to meet up with this time so that the patients will be able to eat before taking their drugs.
Again, they have to dedicate more time spiritually. The rate of prayers needs to increase as they believe that God’s intervention is very important.
Another effect is that some parents fall sick as a consequence of the sickness of their children. Mothers especially do not support the fact that their children are in such condition. Others will fall sick because of sleeplessness in the hospital with patients.
From a social point of view, we can have the following effects:
It is commonly said that the youths are the future of a nation. Schizophrenia is a disease which affects youths greatly.
The disease hinders the continuation of education. It also affects people professionally. When a person is affected he/she will not be able to continue work normally and that will lead to vacancy. Before a replacement is made, the organization will have to suffer for a while.
People in the society tend to be afraid of mental patients, which results at times to prejudice and poor or violent treatments towards the patients.
4. Suggestions for Therapeutic Approaches
At first, I hesitated to include this chapter in my study for a number of reasons. The first was that of established conventions. Conventionally, in this country, only medical practitioners such as doctors, pharmacists and nurses can write medical prescriptions. I am an applied linguist; I have always worked during my study under the supervision of doctors at the psychiatric hospital but this does not make my prescriptions medically or legally valid. Some medical personnel might even consider me to be pretentious. Secondly, the society is wrongly convinced that all health prescriptions must be curative. In actual fact, even among the prescriptions signed by medical practitioners, a large number are preventive rather than curative. And since the slogan “Prevention is better than cure” is in much use today, this has given me courage to write this chapter. In actual fact, during the course of this research, I have noted that while the psychiatrists handled the physical and curative features of the pathology, the applied linguists, while working in close collaboration with the physicians, can make a remarkable contribution regarding the preventive features. And as we are going to point out, the preventive strategies which we are going to present are closely tied up with both the initial and aggravating factors of schizophrenia.
4.1. Strategies Targeting Initial Causes of Schizophrenia
Many researchers hesitate to pinpoint any one cause as the initial cause of this pathology; most tend to mention family history and genetics, environment as well as social factors as causes that combine to trigger off the mental disorders.
4.1.1. Family History and Genetics
Here, the applied linguists insist on general education to sensitize the population regarding the formation of marriage couples. The families should try to check the family histories and genetics before they permit the children to get married. The administration should get involved in implementing these measures; such measures have succeeded in some countries regarding the birth of abnormal children. In actual fact, in many African countries, such steps are often undertaken by parents before they accept the marriages of their children. This has always been looked at as backward by the young generations, but since it will have both a legal and a scientific basis, it can be useful in reducing the number of schizophrenic cases. Young people will stop; they should be careful of whom they want to marry or will eventually marry. They should not marry just any person simply because of good manners, physical beauty or material wealth. If they intend to have children, these children should be protected from being born already predisposed to become schizophrenic. Most of the children born and growing at a given time and in a given zone may undergo trauma some time; but even if most will overcome that trauma, those born by parents both of whom are genetically predisposed to schizophrenia may have 60% of chances to become schizophrenic.
In cases where the future couple cannot be avoided, for individual reasons, such parents should be advised not to have children at all or to avoid exposing such children to traumatic situations that is, poverty, conflicts, etc.
Therefore, such future couples need to undergo series of tests and counseling. This might seem harsh or even costly to an extent, but it is a necessary measure to ensure we have sane parents, sane children, sane families and eventually a sane community.
Young people should be courageous and take the challenge themselves. Youths are the backbone of every society or country. As such, they must be able to take up their responsibilities and make older generation know that they can actually handle sensitive responsibilities appropriately.
4.1.2. Environmental Factors
Even here, the task of the applied linguist is to sensitize the population especially that of the future parents about the dangers children face when they live in a virus infected zone. These viral infections do have a very serious negative impact on the brain development of the child. Many mental disorders which people manifest at the age of puberty are a result of preconception, antenatal or postnatal infections. All the applied linguist can do is to call on all parents, especially the mothers, to avoid all sorts of infections while they still wish to become mothers. These infections could be the result of exposure to dangerous toxins emanating from alcohol, gasoline, tap water, bad toys, etc.
Parents should also be very careful with the sort of friends their children go about with. There are some children who are possessed by bad spirits and they go around recruiting other children into their demonic kingdoms. These possessed children capture others by offering them gifts such as candies, biscuits, rings, necklaces etc. Once a child is in their dragnet, it takes special grace for the child to be liberated. So, it is highly recommended that parents should take great care of their children and strictly control their environment and activities.
4.1.3. Societal Factors
In people who are already predisposed, living in overcrowded and noisy areas, prenatal exposure of the mother to hunger or starvation, living in a stressed family can easily trigger off schizophrenia. Even here, all what the applied linguist can do is to appeal to general educational sensitization. Both the parents and political leaders should face this sensitization. The press and the mass media should do their work. A mother who prefers to buy a pair of shoes of 200,000 Francs and starve her children should be made uncomfortable. A man without a steady income who has three wives all producing children should be called to change. An administration which buys a fleet of Airbus planes without an elementary road network should not be praised. Abject poverty can trigger off schizophrenia in weak brains. Social inequality and segregation may trigger off schizophrenia.
We are all called as nation to uplift the social standard of people. People should be allowed to open businesses with the reduction of taxes or they should even be given a tax free policy for a period of time. Serious war should be waged against corruption and embezzlement and money recovered from guilty parties should be used by the state to improve the living standard of the population by building roads, hospitals, better schools etc.
Youths should be encouraged to be self employed and not to pass several years attempting public entrance examinations that will turn up to be a total source of failure and depression. They should be made to think out of the box and not always wait on the government to do things for them.
Parents also need to observe their children and see what special talents they have so that they can start following special trainings on them from their very tender age. Children should be allowed to choose their path and career with proper follow-up and assistance.
4.1.4. Life Changing Events
Events such as wars, social or political conflicts which are very common today all over the world should be avoided. Under this subtopic we could include the loss of a loved one, rape, loss of a job, a terrible accident, divorce, etc.
The administration should set up special official services to help people in such difficult circumstances.
In all the above mentioned cases, we have given overall strategies which may help to reduce the incidence of schizophrenia or to mitigate its effects in society. The individual case by case strategies will be the work of the medical doctors and nurses in the hospital. The applied linguist will simply accompany them.
4.2. Medical Strategies
Medical strategies are the most complex and they are the reserved domain of psychiatric experts who work in hospital and clinical structures. Applied linguists, like me, simply accompany these specialists so as to learn more about this complex pathology which in many cases will not kill the patients but leaves them personally diminished. And again, it is in this diminished state that the patients may need the help of an applied linguist. The applied linguist will elaborate and apply the interactional strategy that will have a healing effect on the patient. In many cases, most of these patients are frustrated by the feeling that they are considered “mad”, “stupid”, “useless” and even dangerous. Such a negative sentiment of exclusion can push a healing patient to relapse. These patients detest being considered abnormal. They want to be listened to; they want to be talked to as human beings. Of course what they say may be deviant especially from a pragmatic point of view. This is where the applied linguist has to apply his skills. He has to try to make “sense” out of the “nonsense” that the patient is producing. After observing and listening to the patient, the applied linguist will look for and create interesting “topics” that can keep the patient enjoy continuing the conversation. This is not always easy but a creative linguist will find practical solutions that will make the patient feel that he or she is a normal human being. With this attitude, the patient tends to become less aggressive towards other human beings and will be less inclined to relapse into deep schizophrenia.
This is why during my training, I had to accompany the psychiatrist during the consultations, and this gave me room to learn how to interact with patients many of whom were able to recognize me some days later and to continue our previous conversation. It requires a lot of interest and practice but I have learnt that a schizophrenic patient who notes that he or she is accepted and talked to as if he were normal feels very fine after such an interaction. As an applied linguist I learnt how to positively talk to and listen to such patients. One has to avoid contradicting them bluntly even if their discourse may often appear to us illogical. We simply have to try to discover the logic behind these illogical utterances. Such analysis may at times help us to discover the deep origin of the mental disorder and communicate it to the treating doctor. The treating doctor who has to attend to over 20 patients cannot have the liberty to stay down listening to and analyzing utterances of patients. This is the work and even the joy of the applied linguist—to create logic out of illogical utterances of patients.
The linguist does not work alone in isolation; he communicates all his relevant findings to the doctor who will then prescribe the adequate therapeutic strategies. In actual case, the applied linguist should be considered as the laboratory assistant of the treating doctors. He analyzes the pragmatic data of the interactions of the schizophrenic patients, presents and explains it to these doctors who then prescribe the appropriate therapeutic strategies. And on occasions, the strategies may require the presence of the linguist to continue interacting with the patients to assess the progress in the treatment.
5. Conclusion
Although I first underestimated the therapeutic role of Applied Linguists, I end up by convincing myself and everybody that that role needs to figure in this study. The linguist doesn’t work alone on schizophrenic patients; like the nurses and laboratory personnel, he accompanies, advises and helps the treating doctors. He does not make medical prescriptions; some hospital administrators do not see his utility. This chapter shows the important role that linguists can and must play in the hospital towards a schizophrenic patient at the beginning of, during and after a doctor’s intervention.
However it has become obvious after this study that the interventions of the linguist in the handling of schizophrenic patients play a considerable preventive role. When we study and analyse the linguistic communications, we can contribute to the search and finding of strategies that may prevent them relapsing into the pathology. I may conclude that the linguist plays the role of an educator who has to train all the stakeholders in the art of interacting with and understanding the speech of schizophrenic patients. The communication breakdown between the patient and the immediate entourage is a very serious aggravating factor of this pathology. We seem to understand this when it comes to family, social, political or international conflicts; the breakdown of dialogues is very dangerous to peace. In the same way, the breakdown of interaction between the schizophrenic patient and the surrounding communities is very dangerous. Only linguists are trained to interact with these patients. Hence, linguists should be allowed to stay around and help in interacting with the patients.