Correlation of Depression with the Functional Profile of Elderly People Living in Homes for the Aged ()
1. Introduction
Aging refers to a dynamic, progressive and irreversible event related to biological, psychic and social factors in which they trigger structural, physiological and psychological changes as well as social changes in the individual, favoring the development of pathological processes [1].
According to Shumway-Cook and Woollacott (2013), there are two main theoretical lines that study aging: one of them considers the primary aspects related to genetic characteristics and the deterioration of the nervous system and the other the secondary ones, which evaluates the influence of the damages caused by environmental factors, such as radiation, pollution, lifestyle, among others [2].
Due to the growth of the elderly population, there is a notable lack of preparation among family and society members to endure the challenges of this new reality, resulting in the growing demand for the elderly in homes for the aged (HA). The HA is defined as residential, governmental and non-governmental institutions for the collective housing of persons aged 60 and over who may have family support or not [3].
An important aspect related to the institutionalized elderly person is depression, because in HA, the elderly are excluded from living with society and adopt a different lifestyle. This social isolation leads to loss of identity, self-esteem and freedom, solitude and often resulting in a depressive state [4].
The consequences of aging may be risk factors for depression in the elderly, in which the disease is found in 10% of people over 60, according to the united nations of Brazil (2017) [5].
Wannmacher & Lenita in 2017, describe that about 40% of elderly who living in HA have depression [6]. According to the Pan-American health organization (PAHO/WHO, 2018) lack of interest, sadness for long periods and the decline of energy to perform daily activities characterize depressive disorders. Loss of memory, decreased visual acuity, and difficulty in move around add to make older people over 85 years of age more vulnerable to be depressed [5].
Functionality is defined as the ability to manage one’s life or take care of oneself and is the basis of the concept of health for the elderly as well as being the starting point in their evaluation [7] functionality is today the great paradigm of geriatrics and gerontology, because it is necessary to understand how the commitment of physical health, mental health, autonomy, social integration, family support and economic independence can affect the functional capacity of the elderly person who has a long [8] [9].
According to the National Institute of Statistics (2014), about 50% of the population, aged 65 or over, said they had difficulty or could not perform at least one of six daily activities (see, listen, walk, memory/concentration, take bath/dress up, understand/make yourself (understood). In this way, the increase in the prevalence of chronic diseases influences the functional status of the elderly, reducing autonomy and independence [8] [10].
Therefore, the present study aims to describe the correlation between depression and function of elderly people living in homes for the aged.
2. Material and Methods
A cross-sectional and descriptive study of a qualitative approach was carried out with 70 elderly of both sexes, 40 women and 30 men, aged 60 years or older, living in HA of the state of Rio de Janeiro.
The present study was approved in 27/11/2017 by the ethics committee of Unigranrio University (CAAE: 56001116.70000.5646) and is in accordance with resolution 466/2012 and resolution 510/2016. The elderly and their caregivers received a detailed explanation of the evaluation objectives and procedures and signed the informed consent form (ICF) agreeing to voluntarily participate in the research.
The inclusion requirements that were adopted are: elderly of both sexes, aged 60 to 100 years, who did not present severe cognitive impairment (<13) evaluated by the mini mental state examination (MMSE) [11] and who accepted to participate in the study. Elderly individuals who presented auditory alterations and severe cognitive impairment (according to the MMSE criteria) were excluded.
Data collection was carried out from february to april 2018. The visits were pre-scheduled with the heads of the institutions. Ninety interviews were conducted with a duration of approximately 20 minutes.
The sample was initially composed of 90 elderly people, and after the beginning of the collection, it was identified that 18 elderly people presented severe cognitive impairment, 1 elderly didn’t agree to sign the term of free inquiry and 1 elderly had serious hearing alterations, so they were excluded from the sample.
Sociodemographic characterization and questions related to health conditions were carried out through the structured script in the form of interviews, prepared by the researchers. The script included the following independent variables: gender, age, length of institution stay, marital status, offspring, reason for institutionalization, receiving visits, chronic diseases, use of medications, self-perception of health, report of pain, falls in recent months, fear of falls and dispositive to aid of gait.
The functional capacity of the elderly to perform the activities of daily living (ADL) was evaluated through the Katz [12] index, which evaluates the capacity for six basic activities: bathing, dressing, going to the bathroom, transferring from chair to bed and vice versa, control sphincters and feed themselves.
Depressive states were evaluated through the geriatric depression scale (GDS) [13], which is composed of easy-to-understand questions and has a small variation in the response possibilities (yes/no).
3. Results
The description of the general characteristics of the elderly can be observed in Table 1. It showed that there was a predominance of the female gender (57.1%) in relation to the male gender (42.9%). The mean age of the elderly was 74.8 years. It was observed that 41.43% did not complete elementary education, 22.86% had completed secondary education, 18.57% did not study, 10.0% had completed elementary education, 5.71% had completed higher education and only 1.43% had incomplete elementary education. The average length of institution stay calculated in months was 55 months. Half of the elderly were widowers 50.0%, 24.3% were single, 20% were divorced and only 5.70% were married. The average number of children was 1.57 per person.
The conditions of these elderly people in LSIE were observed in Table 2, showing that 48.6% lived in long stay institutions of their own free will, and 54.3% received visits. The majority of the interviewees (64.3%) said they did not present chronic diseases, reported using medication (65.7%), said no to reports of pain (71.4%) and use of gaiters (75%), are afraid of falling (51.4%) and when asked about their self-perception of health, they reported good health (74.3%). Only 24.3% said they had suffered falls in recent months.
![]()
Table 1. Characteristics of LSIEs. identification info.
Table 3 shows the average of the questionnaires. The basic daily life activities (Katz) scale showed that 57 elderly people had the ability to perform basic activities of daily living independently, 5 were moderate dependent and 8 were dependent.
According to the MMSE evaluation, 25 elderly individuals presented moderate cognitive impairment, 27 mild cognitive impairment and 18 without cognitive impairment.
In relation to GDS, 37 elderly had a normal psychological presentation, 27 with mild depression and only 6 with severe depression.
Graph 1 shows a histogram which demonstrate the relationship between the
![]()
Table 3. Avareage of questionnaries applied.
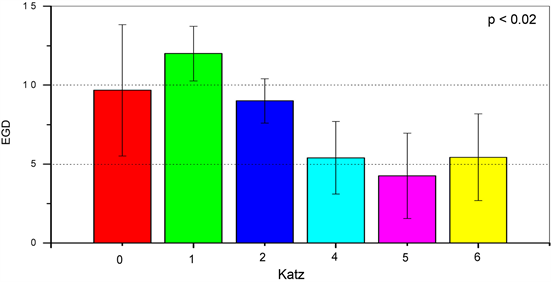
Graph 1. Relationship between the Katz index score and the GDS scale.
Katz index score and the GDS scale. We understand that the lower the Katz index, the higher the GDS, demonstrating a statistically significant relation (p < 0.02). This data suggests that individuals with lower functional level present a greater depressive presentation. This can be better understood in Graph 2.
Graph 2 shows a boxplot that demonstrates the same correlation of Graph 1 but is divided into two groups. The Katz score of 0 - 4 represents a functional profile with total to moderate dependence and the other group, with a score of 5 to 6, representing functional.
Independence. We can affirm through the analysis of this graph that, the elderly with a Katz index of 0 - 4, that is, a functional profile with total to moderate dependence, demonstrate a higher score in the GDS, with an average value of 9, showing a state moderate to severe depression. Moreover, the elderly with a Katz index of 5 - 6, with functional independence, presented an average value of the geriatric depression scale of 5, showing a significant correlation (p < 0.004) that there was no evident depressive state.
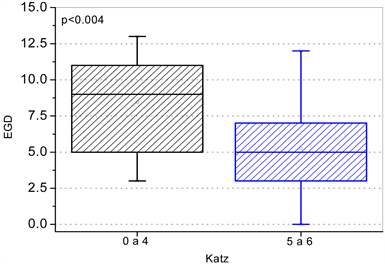
Graph 2. Box graph (boxplot) two level of Katz index with scale GDS.
Graph 1 shows a histogram which demonstrate the relationship between the Katz.
4. Discussion
According to the descriptive analysis presented, there is a predominance of the female gender (57.1%), similar results were found in several studies, including one conducted in the northern brazilian coast of Brazil about the sociodemographic profile, family aspects, health perception, capacity functional and depression in the institutionalized elderly, in which 66.7% were females [14].
According to data from the IBGE in 2014, the life expectancy of women was 78.5 years and the men were 71.2 years. This may be one of the explanations of the greater prevalence of the female gender in HA, in addition to the population in general being composed, for the most part, of women 51.4% [15].
In relation to the marital status, it was verified that many of the institutionalized elderly are widowed, an equivalent response was verified in a study in HA of São Carlos (SP), in which 48% of the sample were widowers, a factor in consonance with our study, and which can be considered a reason for institutionalization [16]. It can also be verified in the present study that the majority of the elderly 65.7% had children, a result that diverges from studies done in HA of Bahia [17].
The average time of institutionalization was 55.1 months, ranging from 3 to 240 months. There were several reasons why the elderly took this decision, considering that 48.6% of hospitalizations were of their own volition, 34.3% were by family decision and 27.1% were homeless.
The study showed that a little more than half of the elderly (54.0%) were visited, corroborating a study on the socioeconomic and epidemiological profile of institutionalized elderly in Brasília in which they presented similar results. About 51% of the elderly received visits from family members and acquaintances [18]. The visit to the institutionalized elderly person discharges the issue of abandonment and contributes to their adaptation to the new environment in which they will reside [16].
Some studies have demonstrated a large percentage of institutionalized elderly people with chronic diseases [18] [19], as well as the use of drugs [20], similar data can be observed in the present study in which 64.3% of the elderly said they had chronic diseases and 65.7% of medicines. The majority of participants reported good health 74.3% and only 14.3% said they considered bad health, the other 11.4% considered their health reasonable. Similar results can be observed in other studies [19].
The minority of the elderly interviewed reported chronic pain 28.6%. These results corroborate the study done in the north coast of Rio Grande do Sul [21], in which only 13.3% of the elderly reported generalized pain. However, other studies show a high prevalence of chronic pain among institutionalized elderly people [22].
Such as one performed in Jequié (Bahia) 73.3%. Pain research is fundamental to determine the measures necessary to promote the well-being and health of the elderly population [22].
The occurrence of falls in institutionalized people or not can have a major negative impact on their mobility, in addition to the risk of developing depression, the elderly may increase their anxiety and fear of falling again, increasing the risk of new occurrences [23].
The study found that only 24.3% of the elderly interviewed suffered falls in recent months. Similar data can be verified in another study [24], where the prevalence of falls was 37.2%.
It can also be verified that in the present study, the group that suffered falls, the majority were female (70.59%), being in accordance with a study carried out in the city of Catanduva (SP) [25], in which 71.4% of the elderly who suffered falls were women.
Despite the low number of elderly people who suffered falls in recent months (24.3%), the study showed that just over half of the elderly are afraid of falling (51.4%) and that of the group that was afraid, most were of the female gender 52.78%. A study done in the city of Santos, SP was similar to the present study, with about 59.3% [26].
Regarding the dispositive to aid the gait, our study showed that only 25% of the elderly interviewed use some type of gait dispositive. Similar to the study done in Belo Horizonte (MG), where 38.3% did not use a gait aid device [19]. Despite the percentage difference, it can be observed that the elderly who use some type of devices to aid gait are the minority (Table 2).
Our study found that the majority of the elderly 81.43% were independent for activities of daily living (ADL). A similar response can be observed in a study carried out in HA located in the city of João Pessoa, where it was observed that the majority of respondents 72.7% had good functional capacity to perform AVD [27]. In the evaluation of the ABVD in the elderly without cognitive decline, carried out in a survey in Belém do Pará, the vast majority were independent [28].
In relation to the depressive state of the institutionalized elderly, our study showed that 52.86% of the elderly did not present depressive symptoms, 38.57% presented mild depression and only 8.57% presented severe depression. This result is according to a study conducted in Curitiba [29], in which 55.54% of the elderly did not present depressive symptoms and 45.45% presented moderate to severe depression, with a mean of 4.68 ± 3.29, which is also in accordance with our study in which the average was 5.86 ± 3.15, values referring to a normal psychological presentation.
Another study carried out in the north of Rio Grande do Sul [30] showed that 57% of the elderly were classified as normal in GDS, 38% had mild depression and 0.5% had severe depression. In the survey conducted in the federal district, 51% of the elderly interviewed had a normal psychological picture, 36.3% were classified as having mild depression and 12.7% were severely depressed. Thus, the investigations investigated, are in accordance with the data found in our research, stating that the majority of the institutionalized elderly do not present a depressive picture.
When we explore the relationship between GDS and the institutionalized elderly functionality evaluated through Katz, we can observe in that the higher the GDS score, the lower the Katz index. That is, the higher the level of depression, the greater the degree of dependence on the elderly. A study carried out in Maceió [31] showed that 65.0% of the institutionalized elderly have depressive symptoms and about 56.3% are dependent for the ABVD, confronting the present study in which the majority of the elderly were independent (81.43%) and had a normal psychological picture (52.86%).
However, it is possible to observe that the correlation between the two scales demonstrates that depressed elderly people are more susceptible to present a reduction in functional capacity. Such a result can also be observed in a review of depressive literature. This demonstrates that depression is associated with the functionality of the institutionalized elderly person.
During the research, we realized that the bedridden elderly people had the most restricted contact and the heads of the institutions limited the interviews with this group. New studies should be performed emphasizing the profile of these individuals, increasing the number of factors associated with depression in institutionalized elderly people, in which the low capacity or functional incapacity for pain was significantly associated with the symptoms of depression in the elderly of HA [32]. Elderly people with depression are more susceptible to demonstrate greater physical and emotional impairment, interfering with quality of life and consequently reducing functional independence [33].
5. Conclusion
The present study showed that there is a greater predominance of the female gender in HA, with an average of 74 years and with an average time of hospitalization of 55 months. The majority of the elderly were independent and a little more than half had a normal psychological picture. In the correlation of the variables depression and functionality, it was verified that the more functional the institutionalized elderly, the lower the chances of presenting the state of the bedridden elderly to verify if there is an increase in the prevalence of depressive elderly and if it is correlated with the functional capacity and autonomy.
Acknowledgements
To the elderly, their relatives, employees and responsible for long-stay institutions that helped and enabled this work to be carried out.